Download
1 / 16
170 likes | 624 Views
High dose inhaled corticosteroids in asthma. Options for local implementation NPC. Key therapeutic topics – Medicines management options for local implementation. Second update July 2011. Review the use of inhaled corticosteroids (ICS) routinely in patients with asthma

E N D
Options for local implementationNPC. Key therapeutic topics – Medicines management options for local implementation. Second update July 2011 • Review the use of inhaled corticosteroids (ICS) routinely in patients with asthma • Step down the dose and use of ICS where clinically appropriate in patients with asthma
Key questions In asthma: • When are ICS recommended? • What are the safety issues with high doses of ICS? • What about the use of high doses of ICS in children? • How should people on high doses of ICS be stepped down? • How are we doing?
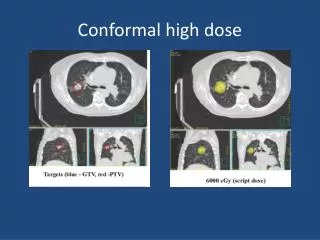
When are ICS recommended?BTS/SIGN British Asthma Guideline, May 2008, Revised May 2011 Consider high dose ICS Standard dose ICS
CSM and guidance for fluticasoneCurrent Problems in Pharmacovigilance, August 2001 For mild asthma starting dose is 100 micrograms twice daily In moderate and severe asthma starting dose may need to be 250 to 500 micrograms twice daily Because of risk of systemic effects, doses above 500 micrograms twice daily should be prescribed only: for patients where additional benefit is expected or demonstrated, or by ability to reduce oral steroid use such doses should be initiated by a specialist in the management of asthma (could be consultant or GP)
Other ICS safety advice from the MHRA/CHM • Prolonged use of high doses of inhaled steroid carries a risk of systemic side-effects, including adrenal suppression or crisis, growth retardation in children and adolescents, decrease in bone mineral density, cataract and glaucoma • Current Problems 2006:5 • In addition to the known systemic effects of inhaled and intranasal corticosteroids, a range of psychological or behavioural effects may also occur. These include psychomotor hyperactivity, sleep disorders, anxiety, depression, and aggression (particularly in children). • Drug Safety Update Sept 2010;4(2):A4
Review regularly and titrate to lowest effective dose If not controlled at maximum dose ICS plus other therapies refer to paediatric asthma specialist: BDP >400 microgram/day (age not stated) BUD >800 microgram/day (under 12 years) FP >400 microgram/day (4 to 16 years) CSM and guidance for ICS and adrenal suppression in childrenCurrent Problems in Pharmacovigilance, October 2002
Inhaled steroids and risk of diabetesSuissa S, et al. Am J Med 2010;123:1001–6, www.npc.nhs.uk/rapidreview/?p=2485 • Cohort study from Quebec health insurance database • Patients treated for respiratory disease 1990–2005 • Risk of onset of diabetes with inhaled steroids, over 5.5 years • Overall RR 1.34, 95% CI 1.29 to 1.39 • With high dose ICS (equivalent to fluticasone ≥1000microg/day) RR 1.64, 95% CI 1.52 to 1.76, NNH = 21 • Risk of diabetes progression from oral therapy to insulin, over 5.5 years • Overall RR 1.34, (95%CI 1.17 to 1.53) • With high dose ICS RR 1.54 (95% CI 1.18 to 2.02) RR Relative risk NNH Number needed to harm
Emma died at the age of 5 from complications of adrenal-suppression, she took between 500 and 2000 micrograms of fluticasone every day for several years. She died in 2001. Sheriff’s Investigation: Criticisms of Emma’s treatment and care Failure to prescribe safely The GP and the consultant were both aware that Emma was taking high levels of the ICS. Both believed that even though this was not ideal, the medication did not pose a threat to Emma’s health Failure to anticipate a rare adverse event Neither Emma’s GP nor her specialist had personal experience of adrenal suppression or adrenal failure in clinical practice, both believed the risk was sufficiently small to be disregarded Failure to challenge marketing messages “GlaxoSmithKline (the drug’s manufacturer) had promoted the drug as the drug of choice for managing severe childhood asthma. The advertising slogans stressed the safety of the drug and its use with children Fatal Accident Inquiry: Death of a child on inhaled fluticasonewww.scotcourts.gov.uk/opinions/FAI_SC.html
Fatal Accident Inquiry: cont… Her brother Calum, who also had asthma and was on FP, was admitted to hospital with serious problems related to adrenal suppression one month after Emma died. Following Calum’s diagnosis, all children and adolescents who had attended Yorkhill Hospital and were receiving inhaled fluticasone (>500 micrograms) would be recalled for synacthen testing: 426 children were identified, of whom 140 were receiving doses of fluticasone outside of licence By the time of testing, only 78 children were receiving doses out of licence, but of these 34 had impaired adrenal function Of all the children tested, 3% had severe impairment of cortisol production and all of these children were asymptomatic All children recalled for testing were evaluated for the potential to reduce their fluticasone dose Those children whose symptoms could not be managed on a lower dose, were kept under regular review at the Children’s Hospital
What about steroid cards?CHM Current Problems May 2006:5 Steroid treatment cards should be routinely provided for patients who require prolonged treatment with high doses of inhaled steroids High dose may be considered as: ‘Off-label’ high doses of inhaled steroids Maximal licensed doses of inhaled steroids when used in conjunction with other steroids (such as oral steroids) Use of inhaled steroids with concomitant medicines that inhibit their metabolism (cytochrome P450 inhibiting drugs: e.g. HIV protease inhibitors) Other high-risk patients should be provided with a steroid card, at the discretion of the prescriber/ pharmacist
Stepping downBTS/SIGN British Asthma Guideline, May 2008, Revised May 2011 ‘Reduction in inhaled steroid dose should be slow as patients deteriorate at different rates’.
Is stepping down possible in practice?Hawkins G, et al. BMJ 2003;326:1115–20 259 ‘stable’ asthma patients in Scotland: on high dose ICS (mean 1430 micrograms BDP or equivalent) randomised to no alteration OR 50% reduction in dose. Followed-up for 1 year: no difference in exacerbations no difference in visits to GP or hospital no difference in health status (SGRQ) Average ‘step-down’ = 25% less ICS (348 micrograms)
How are we doing? (1)GP prescribing of high-dose ICS in childrenThomas M, et al. Br J Gen Pract 2006;56:788–90 ‘This study highlights the over-use of high dose inhaled steroids and the under-use of add-on therapy’
How are we doing? (2)GP prescribing of high-dose ICS in childrenThomas M, et al. Br J Gen Pract 2006;56:788–90 BDP-e ‘Some children were prescribed doses of steroid that risked life-threatening adrenal suppression’
Key messages • ICS are the most effective preventer drug and are safe and effective at standard doses • Patients should be maintained at the lowest possible dose of ICS which effectively controls asthma • Review regularly, particularly those on high doses • Follow MHRA (CSM) advice (particularly relating to children) • Fluticasone potency double that of beclometasone or budesonide • Provide steroid cards routinely for patients on prolonged treatment with high doses of ICS • Step down therapy when asthma is controlled; review patients regularly