Download
1 / 1
10 likes | 110 Views
Physical Medicine and Rehabilitation. RESULTS Relationship to Executive Functioning Measures:. METHODS Participants:

E N D
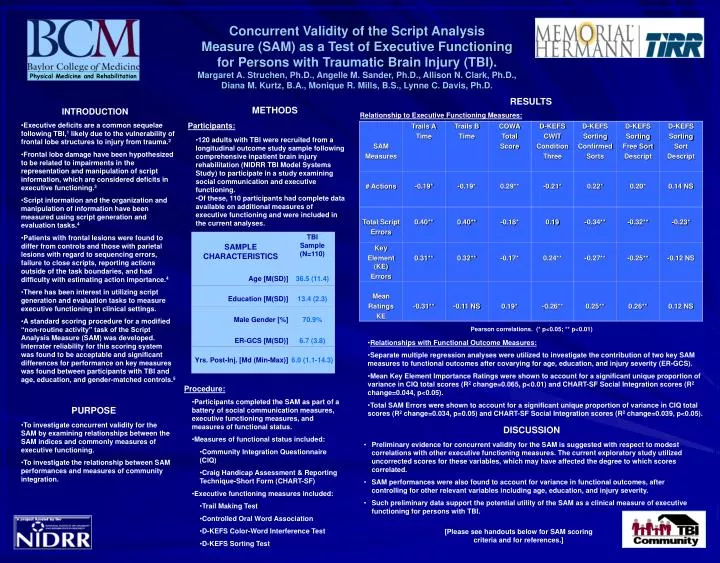
Physical Medicine and Rehabilitation RESULTS Relationship to Executive Functioning Measures: • METHODS • Participants: • 120 adults with TBI were recruited from a longitudinal outcome study sample following comprehensive inpatient brain injury rehabilitation (NIDRR TBI Model Systems Study) to participate in a study examining social communication and executive functioning. • Of these, 110 participants had complete data available on additional measures of executive functioning and were included in the current analyses. • INTRODUCTION • Executive deficits are a common sequelae following TBI,1 likely due to the vulnerability of frontal lobe structures to injury from trauma.2 • Frontal lobe damage have been hypothesized to be related to impairments in the representation and manipulation of script information, which are considered deficits in executive functioning.3 • Script information and the organization and manipulation of information have been measured using script generation and evaluation tasks.4 • Patients with frontal lesions were found to differ from controls and those with parietal lesions with regard to sequencing errors, failure to close scripts, reporting actions outside of the task boundaries, and had difficulty with estimating action importance.4 • There has been interest in utilizing script generation and evaluation tasks to measure executive functioning in clinical settings. • A standard scoring procedure for a modified “non-routine activity” task of the Script Analysis Measure (SAM) was developed. Interrater reliability for this scoring system was found to be acceptable and significant differences for performance on key measures was found between participants with TBI and age, education, and gender-matched controls.5 Concurrent Validity of the Script AnalysisMeasure (SAM) as a Test of Executive Functioning for Persons with Traumatic Brain Injury (TBI).Margaret A. Struchen, Ph.D., Angelle M. Sander, Ph.D., Allison N. Clark, Ph.D., Diana M. Kurtz, B.A., Monique R. Mills, B.S., Lynne C. Davis, Ph.D. Pearson correlations. (* p<0.05; ** p<0.01) • Relationships with Functional Outcome Measures: • Separate multiple regression analyses were utilized to investigate the contribution of two key SAM measures to functional outcomes after covarying for age, education, and injury severity (ER-GCS). • Mean Key Element Importance Ratings were shown to account for a significant unique proportion of variance in CIQ total scores (R2 change=0.065, p<0.01) and CHART-SF Social Integration scores (R2 change=0.044, p<0.05). • Total SAM Errors were shown to account for a significant unique proportion of variance in CIQ total scores (R2 change=0.034, p=0.05) and CHART-SF Social Integration scores (R2 change=0.039, p<0.05). • Procedure: • Participants completed the SAM as part of a battery of social communication measures, executive functioning measures, and measures of functional status. • Measures of functional status included: • Community Integration Questionnaire (CIQ) • Craig Handicap Assessment & Reporting Technique-Short Form (CHART-SF) • Executive functioning measures included: • Trail Making Test • Controlled Oral Word Association • D-KEFS Color-Word Interference Test • D-KEFS Sorting Test • PURPOSE • To investigate concurrent validity for the SAM by examining relationships between the SAM indices and commonly measures of executive functioning. • To investigate the relationship between SAM performances and measures of community integration. • DISCUSSION • Preliminary evidence for concurrent validity for the SAM is suggested with respect to modest correlations with other executive functioning measures. The current exploratory study utilized uncorrected scores for these variables, which may have affected the degree to which scores correlated. • SAM performances were also found to account for variance in functional outcomes, after controlling for other relevant variables including age, education, and injury severity. • Such preliminary data support the potential utility of the SAM as a clinical measure of executive functioning for persons with TBI. [Please see handouts below for SAM scoring criteria and for references.]



















