Download
1 / 1
10 likes | 147 Views
It’s h ard to see what’s not there: A c ase of c ryptorchidism that e volved into i ntra-abdominal m etastatic s eminoma

E N D
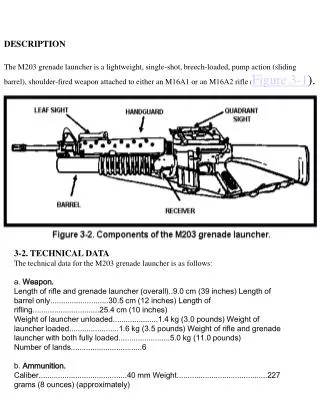
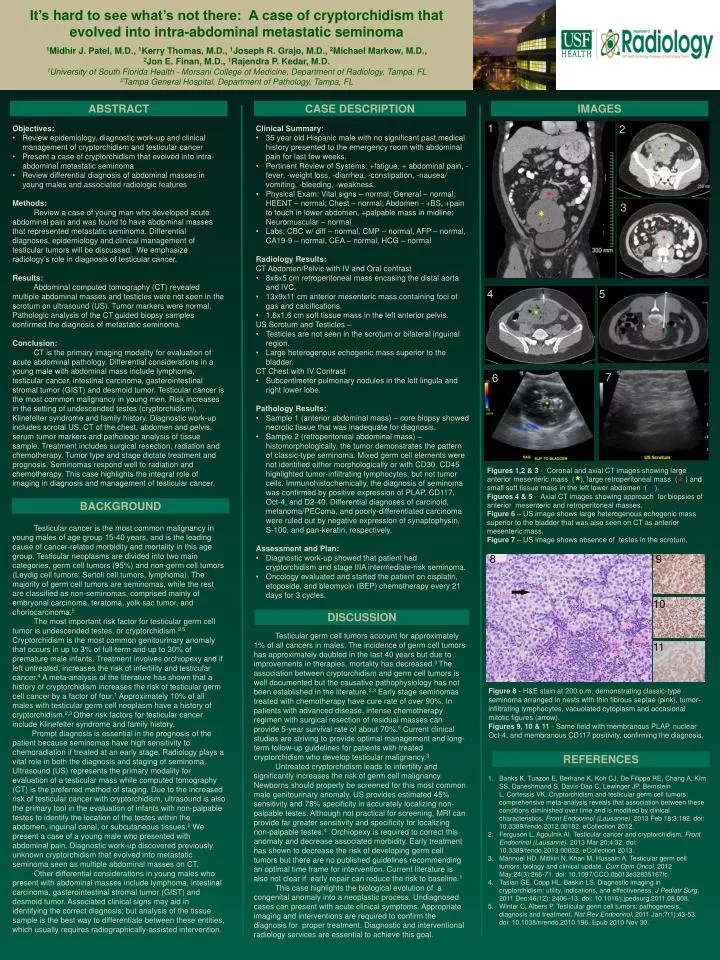
It’s hard to see what’s not there: A case of cryptorchidism that evolved into intra-abdominal metastatic seminoma 1Midhir J. Patel, M.D., 1Kerry Thomas, M.D., 1Joseph R. Grajo, M.D., 2Michael Markow, M.D., 2Jon E. Finan, M.D., 1Rajendra P. Kedar, M.D.1University of South Florida Health - Morsani College of Medicine, Department of Radiology, Tampa, FL2Tampa General Hospital, Department of Pathology, Tampa, FL ABSTRACT CASE DESCRIPTION IMAGES 1 2 • Objectives: • Review epidemiology, diagnostic work-up and clinical management of cryptorchidism and testicular cancer • Present a case of cryptorchidism that evolved into intra-abdominal metastatic seminoma • Review differential diagnosis of abdominal masses in young males and associated radiologic features • Methods: Review a case of young man who developed acute abdominal pain and was found to have abdominal masses that represented metastatic seminoma. Differential diagnoses, epidemiology and clinical management of testicular tumors will be discussed. We emphasize radiology’s role in diagnosis of testicular cancer. • Results: • Abdominal computed tomography (CT) revealed multiple abdominal masses and testicles were not seen in the scrotum on ultrasound (US). Tumor markers were normal. Pathologic analysis of the CT guided biopsy samples confirmed the diagnosis of metastatic seminoma. • Conclusion: CT is the primary imaging modality for evaluation of acute abdominal pathology. Differential considerations in a young male with abdominal mass include lymphoma, testicular cancer, intestinal carcinoma, gasterointestinal stromal tumor (GIST) and desmoid tumor. Testicular cancer is the most common malignancy in young men. Risk increases in the setting of undescended testes (cryptorchidism), Klinefelter syndrome and family history. Diagnostic work-up includes scrotal US, CT of the chest, abdomen and pelvis, serum tumor markers and pathologic analysis of tissue sample. Treatment includes surgical resection, radiation and chemotherapy. Tumor type and stage dictate treatment and prognosis. Seminomas respond well to radiation and chemotherapy. This case highlights the integral role of imaging in diagnosis and management of testicular cancer. • Clinical Summary: • 35 year old Hispanic male with no significant past medical history presented to the emergency room with abdominal pain for last few weeks. • Pertinent Review of Systems: +fatigue, + abdominal pain, -fever, -weight loss, -diarrhea, -constipation, -nausea/ vomiting, -bleeding, -weakness • Physical Exam: Vital signs – normal; General – normal; HEENT – normal; Chest – normal; Abdomen - +BS, +pain to touch in lower abdomen, +palpable mass in midline; Neuromuscular – normal • Labs: CBC w/ diff – normal, CMP – normal, AFP – normal, CA19-9 – normal, CEA – normal, HCG – normal • Radiology Results: • CT Abdomen/Pelvic with IV and Oral contrast • 8x6x5 cm retroperitoneal mass encasing the distal aorta and IVC. • 13x9x11 cm anterior mesenteric mass containing foci of gas and calcifications. • 1.6x1.6 cm soft tissue mass in the left anterior pelvis. • US Scrotum and Testicles – • Testicles are not seen in the scrotum or bilateral inguinal region. • Large heterogenous echogenic mass superior to the bladder. • CT Chest with IV Contrast • Subcentimeter pulmonary nodules in the left lingula and right lower lobe. • Pathology Results: • Sample 1 (anterior abdominal mass) – core biopsy showed necrotic tissue that was inadequate for diagnosis. • Sample 2 (retroperitoneal abdominal mass) –histomorphologically, the tumor demonstrates the pattern of classic-type seminoma. Mixed germ cell elements were not identified either morphologically or with CD30. CD45 highlighted tumor-infiltrating lymphocytes, but not tumor cells. Immunohistochemically, the diagnosis of seminoma was confirmed by positive expression of PLAP, CD117, Oct-4, and D2-40. Differential diagnoses of carcinoid, melanoma/PEComa, and poorly-differentiated carcinoma were ruled out by negative expression of synaptophysin, S-100, and pan-keratin, respectively. • Assessment and Plan: • Diagnostic work-up showed that patient had cryptorchidism and stage IIIA intermediate-risk seminoma. • Oncology evaluated and started the patient on cisplatin, etoposide, and bleomycin (BEP) chemotherapy every 21 days for 3 cycles. 3 4 5 7 6 Figures 1,2 & 3 - Coronal and axial CT images showing large anterior mesenteric mass ( ), large retroperitoneal mass ( ) and small soft tissue mass in the left lower abdomen ( ). Figures 4 & 5 - Axial CT images showing approach for biopsies of anterior mesenteric and retroperitoneal masses. Figure 6 – US image shows large heterogenous echogenic mass superior to the bladder that was also seen on CT as anterior mesenteric mass. Figure 7 – US image shows absence of testes in the scrotum. * * * BACKGROUND Testicular cancer is the most common malignancy in young males of age group 15-40 years, and is the leading cause of cancer-related morbidity and mortality in this age group. Testicular neoplasms are divided into two main categories, germ cell tumors (95%) and non-germ cell tumors (Leydig cell tumors, Sertoli cell tumors, lymphoma). The majority of germ cell tumors are seminomas, while the rest are classified as non-seminomas, comprised mainly of embryonal carcinoma, teratoma, yolk sac tumor, and choriocarcinoma.5 The most important risk factor for testicular germ cell tumor is undescended testes, or cryptorchidism.2,5 Cryptorchidism is the most common genitourinary anomaly that occurs in up to 3% of full-term and up to 30% of premature male infants. Treatment involves orchiopexy and if left untreated, increases the risk of infertility and testicular cancer.4 A meta-analysis of the literature has shown that a history of cryptorchidism increases the risk of testicular germ cell cancer by a factor of four.1Approximately 10% of all males with testicular germ cell neoplasm have a history of cryptorchidism.2,3 Other risk factors for testicular cancer include Klinefelter syndrome and family history. Prompt diagnosis is essential in the prognosis of the patient because seminomas have high sensitivity to chemoradiation if treated at an early stage. Radiology plays a vital role in both the diagnosis and staging of seminoma. Ultrasound (US) represents the primary modality for evaluation of a testicular mass while computed tomography (CT) is the preferred method of staging. Due to the increased risk of testicular cancer with cryptorchidism, ultrasound is also the primary tool in the evaluation of infants with non-palpable testes to identify the location of the testes within the abdomen, inguinal canal, or subcutaneous tissues.2 We present a case of a young male who presented with abdominal pain. Diagnostic work-up discovered previously unknown cryptorchidism that evolved into metastatic seminoma seen as multiple abdominal masses on CT. Other differential considerations in young males who present with abdominal masses include lymphoma, intestinal carcinoma, gasterointestinal stromal tumor (GIST) and desmoid tumor. Associated clinical signs may aid in identifying the correct diagnosis; but analysis of the tissue sample is the best way to differentiate between these entities, which usually requires radiographically-assisted intervention. 8 9 10 DISCUSSION Testicular germ cell tumors account for approximately 1% of all cancers in males. The incidence of germ cell tumors has approximately doubled in the last 40 years but due to improvements in therapies, mortality has decreased.3 The association between cryptorchidism and germ cell tumors is well documented but the causative pathophysiology has not been established in the literature.2,3Early stage seminomas treated with chemotherapy have cure rate of over 90%. In patients with advanced disease, intense chemotherapy regimen with surgical resection of residual masses can provide 5-year survival rate of about 70%.5 Current clinical studies are striving to provide optimal management and long-term follow-up guidelines for patients with treated cryptorchidism who develop testicular malignancy.3 Untreated cryptorchidism leads to infertility and significantly increases the risk of germ cell malignancy. Newborns should properly be screened for this most common male genitourinary anomaly. US provides estimated 45% sensitivity and 78% specificity in accurately localizing non-palpable testes. Although not practical for screening, MRI can provide far greater sensitivity and specificity for localizing non-palpable testes.4 Orchiopexy is required to correct this anomaly and decrease associated morbidity. Early treatment has shown to decrease the risk of developing germ cell tumors but there are no published guidelines recommending an optimal time frame for intervention. Current literature is also not clear if early repair can reduce the risk to baseline.1 This case highlights the biological evolution of a congenital anomaly into a neoplastic process. Undiagnosed cases can present with acute clinical symptoms. Appropriate imaging and interventions are required to confirm the diagnosis for proper treatment. Diagnostic and interventional radiology services are essential to achieve this goal. 11 Figure 8 - H&E stain at 200 o.m. demonstrating classic-type seminoma arranged in nests with thin fibrous septae (pink), tumor-infiltrating lymphocytes, vacuolated cytoplasm and occasional mitotic figures (arrow). Figures 9, 10 & 11 - Same field with membranous PLAP, nuclear Oct-4, and membranous CD117 positivity, confirming the diagnosis. REFERENCES • Banks K, Tuazon E, Berhane K, Koh CJ, De Filippo RE, Chang A, Kim SS, Daneshmand S, Davis-Dao C, Lewinger JP, Bernstein L, Cortessis VK. Cryptorchidism and testicular germ cell tumors: comprehensive meta-analysis reveals that association between these conditions diminished over time and is modified by clinical characteristics. Front Endocrinol (Lausanne). 2013 Feb 18;3:182. doi: 10.3389/fendo.2012.00182. eCollection 2012. • Ferguson L, Agoulnik AI. Testicular cancer and cryptorchidism. Front Endocrinol (Lausanne). 2013 Mar 20;4:32. doi: 10.3389/fendo.2013.00032. eCollection 2013. • Mannuel HD, Mitikiri N, Khan M, Hussain A. Testicular germ cell tumors: biology and clinical update. CurrOpinOncol. 2012 May;24(3):266-71. doi: 10.1097/CCO.0b013e32835167fc. • Tasian GE, Copp HL, Baskin LS. Diagnostic imaging in cryptorchidism: utility, indications, and effectiveness. J Pediatr Surg. 2011 Dec;46(12): 2406–13. doi: 10.1016/j.jpedsurg.2011.08.008. • Winter C, Albers P. Testicular germ cell tumors: pathogenesis, diagnosis and treatment. Nat Rev Endocrinol. 2011 Jan;7(1):43-53. doi: 10.1038/nrendo.2010.196. Epub 2010 Nov 30.