Download
1 / 44
570 likes | 1.63k Views
CPD & Dystocia. Adly Nanda Andreas Kurniawan Gregorius Tanamas. Anatomy of Pelvic. Types of Pelvic. Pelvic Inlet. Konjugata AP (Obstetric/Vera). Konjugata Transversal. Konjugata Diagonal (Oblique). Anteroposterior Diameter of Pelvic Inlet.

E N D
CPD & Dystocia Adly Nanda Andreas Kurniawan GregoriusTanamas
Pelvic Inlet Konjugata AP (Obstetric/Vera) Konjugata Transversal Konjugata Diagonal (Oblique)
Anteroposterior Diameter of Pelvic Inlet • Obstetrical conj = diagonal conj -1.5/2 cm • Depends on the height and inclination of the symphysis pubis. • diagonal conjugate >11.5 cm adequate size for vaginal delivery of a normal-sized fetus.
Pelvic Outlet Distansia Tuberum (10,5 cm) Sacrum To Pubic
Maharaj et.al OBSTETRICAL AND GYNECOLOGICAL SURVEY Volume 65, Number 6
Obstruction Chaabra S, et al, Journal of Obstetrics and Gynaecology (2000) Vol. 20, No. 2, 151± 153
Pelvimetry • Bimanual examination (clinical pelvimetry) • X-ray • CT Scan • MRI • radiologic pelvimetry: • there is poor correlation with the clinical outcome of labor, skill-depended (Maharajet,a.l, 2010) • The role of pelvimetry in current obstetric practice is controversial. It has been widely used without adequate RCT (Morrison et al., 1995).
What is adequate pelvis? Maharaj et.al OBSTETRICAL AND GYNECOLOGICAL SURVEY Volume 65, Number 6, 2010
Dystocia • ‘difficult labor’ • characterized by abnormally slow progress of labor. • common if there is disproportion between the presenting part of the fetus and the birth canal. • American College of Obstetricians and Gynecologists : • 1. Abnormalities of the powers (uterine contractility and maternal expulsive effort). • 2. Abnormalities involving the passenger (the fetus). • 3. Abnormalities of the passage (the pelvis).
Common Clinical Findings in Women with Ineffective Labor • Inadequate cervical dilation or fetal descent • Protracted labor—slow progress • Arrested labor—no progress • Inadequate expulsive effort—ineffective "pushing" • Fetopelvic disproportion • Excessive fetal size • Inadequate pelvic capacity • Malpresentation or position of the fetus • Ruptured membranes without labor
Nulipara Taken from http://emedicine.medscape.com/article/273053-media
Multipara Taken from http://emedicine.medscape.com/article/273053-media
Abnormal Labor Indicators Taken from http://emedicine.medscape.com/article/273053-overview
Patophysiology mechanical dystocia Passenger • produce abnormal labor because of the infant's size or from malpresentation. Passage/pelvis • abnormal labor because its contours may be too small or narrow to allow passage of the infant.
Patophysiology functional dystocia power • the frequency and intensity of contractions. • Disruption of communication between adjacent segments of the uterus resulting from surgical scarring, fibroids, or other conduction disruption. • fails to result in cervical effacement and dilation. This is called • Uterine contractile force quantified by the use of an intra-uterine pressure catheter in Montevideo units (MVUs). • Adequate force >200 MVUs during a 10-minute contraction period.
Intrauterine pressure catheter The ACCU-TRACE™ Intrauterine Pressure Catheter Taken from http://www.umm.edu/pregnancy/000138.htm
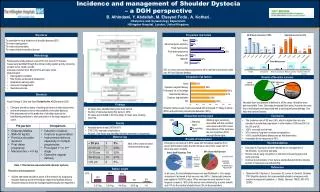
frequency • Of all cephalic deliveries, 8-11% are complicated by an abnormal first stage of labor. Dystocia occurs in 12% of deliveries in women without a history of prior cesarean delivery
Cause Prolonged latent phase • Prolonged: >20 hours in nulliparas ; >14 hours in multiparas. • The most common reason entering labor without substantial cervical effacement. Power • uterine contractility x frequency Montevideo units (MVUs) • Adequate uterine contractile force : >200 MVUs/10 min Passage • The shape of the bony pelvis (eg, anthropoid or platypelloid) • extremely short or obese patient • Patients with history of prior severe trauma to the bony pelvis Passenger • the size & presentation • Fetal macrosomia and other anomalies (including hydrocephalus, encephalocele, or any other abnormality that increases the size of the infant)
Uterine muscle dysfunction • Cause: overdistention due to excessive fetal size and/or uterine fatigue when labor is obstructed by inadequate pelvic capacity, excessive fetal size, or both. • uterine dysfunction VS fetopelvic disproportion interlinked • uterine dysfunction corrected with oxytocin vaginal delivery • “clinicians must rely on a trial of labor to determine if labor can be successful in effecting vaginal delivery” (Williams Obstetrics, 21sted)
hypotonic uterine dysfunction • More common there is no basal hypertonus and uterine contractions have a normal gradient pattern • the slight rise in pressure during a contraction is insufficient to dilate the cervix. • Weak his, frequency ↓ • Cause: anemia, dilated uterus (hydramnion, gemelli, makrosomia, etc) • Divided into • Primary uterine inertia (early laten phase) • Secondary uterine inertia (active 1st stage 2nd stage of labor) • Treatment: monitor general condition, oxytocin (no CPD exist) • CPD SC
hypertonic uterine dysfunction • hypertonic (incoordinate) uterine dysfunction either basal tone is elevated or the pressure gradient is distorted • contraction of the midsegment uterus > fundus • complete asynchronism of the impulses. • Strong his, continuing patient feels pain; hypoxia on fetus • Cause: excess oxytocin • treatment: tocolytic agent, SC
Shoulder Dystocia • diagnosed as such when maneuvers were required to deliver the shoulders in addition to downward traction and episiotomy • Risk Factor • Several maternal risk factors, including obesity, multiparity, and diabetes, all exert their effects because of associated increased birthweight • postterm pregnancy • Intrapartum complications associated with shoulder dystocia include midforceps delivery and prolonged first- and second-stage labor (still controversial)
The American College of Obstetricians and Gynecologists (2002) has concluded that performing cesarean deliveries for all women suspected of carrying a macrosomic fetus is not appropriate, except possibly for estimated fetal weights over 5000 g in nondiabetic women and over 4500 g in those with diabetes.
Consequences • Mother • Postpartum hemorrhage, usually from uterine atony, but also from vaginal and cervical lacerations, is the major maternal risk • Fetus • fetal morbidity and even mortality • 2/3 Transient Erb or Duchenne brachial plexus palsies were the most common injury • clavicular fractures • humeral fractures
Management diagnosis Stop the head traction, immediately call for help McRobert Maneuver (episiotomy if necessary , suprapubic pressure, head traction Maneuver Rubin ( McRobert position, shoulder rotation, suprapubic pressure, head traction) Bear the posterior shoulder, or crawling position or Wood manuever
Cephalopelvic Disproportion • Mismatch between the size of the fetal head and size of the maternal pelvis, resulting in “failure to progress” in labor for mechanical reasons. (Maharaj, D, 2010) • Fetal head : hydrocephalus, Occipito-Posterior malposition • Maternal pelvis : abnormally small / unusual shape. • childhood rickets • Orthopaedic disorders
In such cases the fetal and pelvic dimensions are not abnormal but the presenting diameter of a deflexed O.P. malposition is greater than an occipito-anterior position and labour may become obstructed. • In such cases the term Relative Disproportion is used and in subsequent pregnancies vaginal delivery might reasonably be allowed.
Diagnosis • CPD may only be reliably diagnosed during labour. • Typically the first stage of labour will be prolonged. • Sign • failure of descent of the head VT/abdominal exam • Moulding fetal skull bones override each other. • The parietal bones override each other commonly and both overlie the frontal bones, irreducible • Caput formation oedematous is a feature of the duration of labour rather than CPD.
Occipito Posterior Position • Occipito-posterior position is a malposition of the head and occurs in 13% of vertex presentations. • The presenting part is the vertex and the denominator is the occiput.
references • Cunningham F.G. (Editor), et.al. Williams Obstetrics 21st ed. New York: McGraw-Hill Professional. 2001 • Hanretty KP. Obstetric Illustrated ed.6th. New York: Churcill Livingstone: 2003. p268 • Joy S. Abnormal Labor. 2009. Downloaded from http://emedicine.medscape.com/article/273053-overview