Download
1 / 11
110 likes | 279 Views
Scaling Up Misoprostol for Community-Based Prevention of Postpartum Hemorrhage in Bangladesh Dr. Tapash Ranjan Das PM (MCH) & Deputy Director (MCH), DGFP & Dr. Abu Jamil Faisel Project Director, Mayer Hashi project (an Associate Award of the RESPOND project) &

E N D
Scaling Up Misoprostol for Community-Based Prevention of Postpartum Hemorrhage in Bangladesh Dr. Tapash Ranjan Das PM (MCH) & Deputy Director (MCH), DGFP & Dr. Abu Jamil Faisel Project Director, Mayer Hashi project (an Associate Award of the RESPOND project) & Country Representative EngenderHealth Bangladesh
Background • The maternal mortality rate in Bangladesh decreased from 322 deaths per 100,000 live births in 2001 to 194 per 100,000 in 2010. • Postpartum hemorrhage (PPH) is still the leading cause of maternal death (31% in 2010). • Facility deliveries increased from 15% in 2001 to 23% in 2010. • The government emphasizes the use of community skilled birth attendants (CSBAs) for home births and the development of a midwifery cadre to increase skilled attendance at facilities. • EngenderHealth, through the USAID-funded Mayer Hashi project, supports the Ministry of Health and Social Welfare in preventing PPH through a two-pronged approach: • Active management of the third stage of labor (AMTSL) at the facility level in 21 low-performing districts • Community-based distribution and use of misoprostol (Ref: BMMS 2001 and 2010)
Major Milestones • Establishment of the National PPH Prevention Task Force, Secretariat at EngenderHealth (October 2006) • Approval of misoprostol for prevention of PPH by the Directorate General of Drug Administration and its inclusion in the updated essential drug list (May 2008) • Approval of the piloting of community-based distribution of misoprostol using fieldworkers (August 2008) • Agreement and approval of the effective misoprostol dose for preventing PPH for national use—400 mcg (March 2010) • Approval of the scale-up plan for misoprostol by the National Technical Committee (NTC) of Directorate General of Family Planning (DGFP) (May 2010) • Approval of the national scale-up plan developed with technical assistance from EngenderHealth (September 2010)
Pilot Phase • 1st pilot: Tangail District (Nov. 2008–June, 2009) • Implemented by DGFP, DGHS, and NGOs • Technical assistance, training, monitoring, and misoprostol distribution by EngenderHealth • Formal evaluation of Tangail pilot (Oct. 2009) • 2nd pilot: Cox’s Bazar (Nov. 2009–Mar. 2011) Mayer Hashi project: • Transferred skills and developed skills of DGFP and DGHS to implement pilot • Conducted training of trainers and provided on-site technical assistance to conduct training and orientation • Misoprostol distributed through govt. system • All misoprostol tablets donated by Venture Strategies Innovations; produced locally
Implementation Strategy • Training of all fieldworkers (one day) • Identification and registration of pregnant women by trained government and NGO fieldworkers • Counseling and education by the fieldworkers of pregnant women, their intended birth attendants, and family members, using behavior change communication (BCC) materials • Raising of community awareness through BCC activities and courtyard meetings, with emphasis on facility delivery • Distribution of misoprostol tablets by government/NGO fieldworkers • Follow-up of postpartum women by government/NGO fieldworkers • Back-up of fieldworkers by trained facility-based health care providers, for management of complications
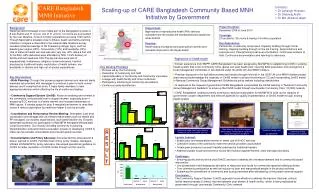
Results of Pilot Programs Tangail: • 71% of the expected pregnant women were registered. • Among them, of those who delivered at home, 94% used misoprostol. • There were no reported cases of misuse. • 0.4% (39) of users reported minor side effects (fever, shivering). • 0.3% (25) of users reported complications (retained placenta, PPH due to other cause) and were referred to hospital. • An estimated nine maternal deaths were averted by the use of misoprostol. Cox’s Bazar: • 69% of expected pregnant women were registered. • Among them, of those who delivered at home, 95% used misoprostol. • There were no reported cases of misuse. • 0.8% (134) of users reported minor side effects (fever, shivering). • 0.1% (26) of users reported complications (retained placenta, PPH due to other cause)and were referred to hospital. • An estimated 10 maternal deaths were averted by misoprostol use. • Four women died at home due to obstructed labor and mishandling by TBA.
Lessons Learned • Misoprostol can be effectively distributed through trained and supervised fieldworkers. • One-day training was found to be sufficient for the fieldworkers. • Service provider attendance is not required during misoprostol use, and well-counseled women themselves can correctly use misoprostol to prevent PPH. • Misoprostol can reduce PPH compared to previous delivery, as reported by the clients. • Delivery attendants need to be educated on misoprostol’s benefits, so they will not prevent women from using the tablets. • A few women reported misoprostol-induced side effects. • The distribution of misoprostol after 32 weeks pregnancy is advisable. • Close collaboration with the government, through implementation of pilots and provision of scientific evidence and continuous technical assistance, increases the chances of developing scalable programs.
Challenges • Raising community awareness about misoprostol use and removing myths and misperceptions about delivery and PPH • Registering and reaching all pregnant women for misoprostol distribution • Ensuring the accuracy and consistency of information provided through the government’s cascade training • Ensuring that women use misoprostol, through consistent monitoring, supervision, and follow-up • Ensuring the reporting of misoprostol use through the government’s management information system • Ensuring a continuous supply of misoprostol for prevention of PPH • Preventing inappropriate use once misoprostol is available countrywide
National Scale-Up • Incorporated misoprostol into the Health, Population and Nutrition Sector Development Program and Operational Plans (2011–2016) • Allocated budget in the Operational Plans for implementation of scale-up • Developed implementation modalities for both DGFP and DGHS • Sent out implementation guidelines/circulars to both DGFP and DGHS field staff • Tested training and BCC materials approved by DGFP and DGHS and handed over by Mayer Hashi • Planned for a phased scale-up, and in July 2011 began scale-up in four districts, with technical assistance from Mayer Hashi • Currently processing bulk procurement of misoprostol tablets