Download
1 / 1
60 likes | 333 Views
Advanced Care Planning: Improving the Quality of End Of Life Care. Dr Emily Guilhem *, Dr Sophie Merrick* & Dr Lulu Kreeger . Kingston Hospital Foundation trust. emily.guilhem@doctors.org.uk (*Joint first authors). Method Cycle 1 :

E N D
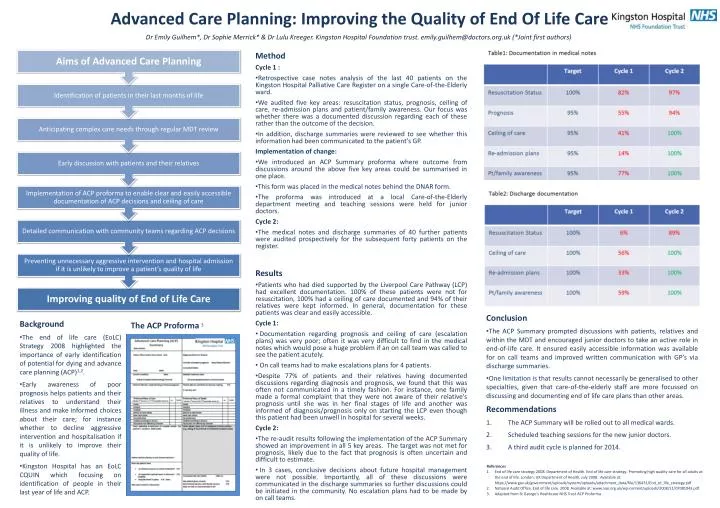
Advanced Care Planning: Improving the Quality of End Of Life Care Dr Emily Guilhem*, Dr Sophie Merrick* & Dr Lulu Kreeger. Kingston Hospital Foundation trust. emily.guilhem@doctors.org.uk (*Joint first authors) • Method • Cycle 1 : • Retrospective case notes analysis of the last 40 patients on the Kingston Hospital Palliative Care Register on a single Care-of-the-Elderly ward. • We audited five key areas: resuscitation status, prognosis, ceiling of care, re-admission plans and patient/family awareness. Our focus was whether there was a documented discussion regarding each of these rather than the outcome of the decision. • In addition, discharge summaries were reviewed to see whether this information had been communicated to the patient’s GP. • Implementation of change: • We introduced an ACP Summary proforma where outcome from discussions around the above five key areas could be summarised in one place. • This form was placed in the medical notes behind the DNAR form. • The proforma was introduced at a local Care-of-the-Elderly department meeting and teaching sessions were held for junior doctors. • Cycle 2: • The medical notes and discharge summaries of 40 further patients were audited prospectively for the subsequent forty patients on the register. • Results • Patients who had died supported by the Liverpool Care Pathway (LCP) had excellent documentation. 100% of these patients were not for resuscitation, 100% had a ceiling of care documented and 94% of their relatives were kept informed. In general, documentation for these patients was clear and easily accessible. • Cycle 1: • Documentation regarding prognosis and ceiling of care (escalation plans) was very poor; often it was very difficult to find in the medical notes which would pose a huge problem if an on call team was called to see the patient acutely. • On call teams had to make escalations plans for 4 patients. • Despite 77% of patients and their relatives having documented discussions regarding diagnosis and prognosis, we found that this was often not communicated in a timely fashion. For instance, one family made a formal complaint that they were not aware of their relative’s prognosis until she was in her final stages of life and another was informed of diagnosis/prognosis only on starting the LCP even though this patient had been unwell in hospital for several weeks. • Cycle 2: • The re-audit results following the implementation of the ACP Summary showed an improvement in all 5 key areas. The target was not met for prognosis, likely due to the fact that prognosis is often uncertain and difficult to estimate. • In 3 cases, conclusive decisions about future hospital management were not possible. Importantly, all of these discussions were communicated in the discharge summaries so further discussions could be initiated in the community. No escalation plans had to be made by on call teams. Conclusion • The ACP Summary prompted discussions with patients, relatives and within the MDT and encouraged junior doctors to take an active role in end-of-life care. It ensured easily accessible information was available for on call teams and improved written communication with GP’s via discharge summaries. • One limitation is that results cannot necessarily be generalised to other specialties, given that care-of-the-elderly staff are more focussed on discussing and documenting end of life care plans than other areas. Recommendations • The ACP Summary will be rolled out to all medical wards. • Scheduled teaching sessions for the new junior doctors. • A third audit cycle is planned for 2014. • Background • The end of life care (EoLC) Strategy 2008 highlighted the importance of early identification of potential for dying and advance care planning (ACP)1,2. • Early awareness of poor prognosis helps patients and their relatives to understand their illness and make informed choices about their care; for instance whether to decline aggressive intervention and hospitalisation if it is unlikely to improve their quality of life. • Kingston Hospital has an EoLC CQUIN which focusing on identification of people in their last year of life and ACP. The ACP Proforma3 • References • End of life care strategy 2008. Department of Health. End of life care strategy: Promoting high quality care for all adults at the end of life. London: UK Department of Health, July 2008. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/136431/End_of_life_strategy.pdf • National Audit Office. End of life care. 2008. Available at: www.nao.org.uk/wp-content/uploads/2008/11/07081043.pdf • Adapted from St George’s Healthcare NHS Trust ACP Proforma