Download
1 / 41
580 likes | 1.08k Views
Intermittent self catheterisation. Presented by. Karen Ayers. Continence Nurse Specialist. Overview. Guidance Where and when it all began Why the bladder sometimes doesn’t empty properly What to consider when teaching ISC Choosing the right catheter

E N D
Intermittent self catheterisation.Presented by Karen Ayers.Continence Nurse Specialist
Overview. Guidance Where and when it all began Why the bladder sometimes doesn’t empty properly What to consider when teaching ISC Choosing the right catheter Men and women what’s the difference (if you don’t know perhaps you’re in the wrong job!) How to know how often to do it Advantages and disadvantages of ISC
Catheter care – RCN guidance for nurses RCN Skills for Health Coloplast Launched March 2008 (Currently being revised)
Competence • You must have the knowledge and skills for safe and effective practice when working without direct supervision • You must recognise and work within the limits of your competence • You must keep your knowledge and skills up to date throughout your working life • You must deliver care based on the best available evidence or best practice (NMC 2008)
Accountability The state of being accountable; liability to be called on to render an account; the obligation to bear the consequences for failure to perform as expected Registered practitioners are accountable to regulatory and professional bodies in terms of standards of practice and patient care (RCN 2006) We will make the NHS more accountable to patients (DH 2010)
RCN guidance 6 competencies • Insert and secure urethral catheters • Monitor, and help individuals to self monitor urethral catheters • Manage suprapubic catheters • Undertake a trial without catheter (TWOC) • Enable individuals to carry out intermittent self catheterisation (ISC) • Review catheter care
Legislation, policy and good practice Competence Documentation Anatomy and physiology Consent Reasons for catheterisation Risk assessment Equipment Catheter care, review and follow-up Patient education Medication and catheterisation Infection control Environmental considerations Healthcare assistants RCN guidance (2008)
Legislation, policy and good practice • CG 2: Infection Control (NICE, 2003) • Catheter Care Guidance for Nurses (RCN, 2008) • Essential Steps to safe, clean care – Urinary catheter care (DH, 2006) • NHS Quality Improvement Scotland: Best Practice Statement, Urinary Catheterisation and Catheter Care, (2004) • EPIC 2 (2007) • National Occupational Standards (Skills for Health) (2008) • Saving Lives: reducing infection, delivering clean safe care. (DH, 2007) • CG40 Urinary incontinence, the management of urinary incontinence in women. (NICE 2006) • The Mental Capacity Act (DH 2005)
Skills for health • All users of all competencies must ensure that practice reflects up to date information and policies • Therefore all services and clinicians must have easy access to up-to-date policies and guidance www.skillsforhealth.org.uk
K6. an in-depth understanding of the causative factors which determine the need for urinary catheter usage K7. an in-depth understanding of why a risk assessment prior to the decision to catheterise or use an intermittent catheter is important and what contributes to this K8. an in-depth understanding of how to advise individuals who undertake intermittent catheterisation K9. an in-depth understanding of the effects of intermittent catheterisation and dilatation on the individual’s comfort and dignity, and ways of handling this K10. an in-depth understanding of the adverse effects and potential complications during urinary catheterisation/dilatation and appropriate actions to take K11. an in-depth understanding of the short and long term risks and health implications associated with intermittent catheterisation/dilatation and how to resolve or minimise these K12. an in-depth understanding of the clinical decisions and method/s required to terminate the usage of intermittent catheterisation/dilatation in an effective and safe manner K13. an in-depth understanding of how individuals should risk assess themselves and how this will influence their self care K14. an in-depth understanding of when to not proceed or abandon catheterisation for an individual and what actions to take CCO6 Knowledge and Understanding
RCN guidance • Assess the individual for ISC, not on their residual urine alone • Renal function, symptom severity and physical and psychological ability to perform ISC must also be considered • Cognitive ability should be assessed • ISC should be considered when TWOC fails
Consent • Mental Capacity Act (2005) 5 key principles • Documentation of the giving of consent for catheter usage and ongoing catheter care is vital from a professional, ethical and legal perspective • Explain rationale for ISC • Explain intended benefits and potential risks • Explain frequency of procedure and that it may be lifelong • Explain the need for follow-up and review (RCN 2008)
Where it all began • Intermittent catheterisation is far from being a modern idea.
Clean Intermittent Self Catheterisation • Lapides an American urologist first pioneered CISC in 1970s • Clean as opposed to sterile catheterisation did not increase the incidence of renal damage or UTI (Lapides et al 1972,1974,1976)
Some causes of incomplete bladder emptying • Neurogenic • Detrusor areflexia • Hyporeflexia • Detrusor-sphincter dyssynergia • Detrusor hyperreflexia
Other causes of incomplete emptying • Enlargement of the prostate • Urethral stricture after an infection or trauma. • Stenosis following surgery of the bladder neck. • Surgical procedures eg. colposuspension or clam cystoplasty. • Constipation • Bladder diverticula and other abnormalities
Who may benefit from ISC ? • Short term • Acute or chronic retention of urine • Awaiting TURP/TWOCS • Post epidural (labour) • Pre/ post pelvic surgery • SUI surgery
Long term • Neurological diseases • Botox • Detrusor failure • Spinal cord injury • Urethral stricture • Congenital neuropathy Residual 100mls or over (5-90yrs) is no barrier to ISC
Other considerations for ISC • Residual volume >10% 0f bladder capacity • Residual Volume >1000mls! • Good manual dexterity and eyesight • Motivation • Support from a regular carer/partner for some • Appropriate follow up support available (Baron, 2000)
Why ISC/CISC? Lapides Viewpoint • To prevent or overcome infection, you need to empty the bladder regularly – CIC • No real increased infection rate using clean versus sterile • CIC promotes “normal” filling andemptying stages of micturition • Upper tract damage limitation • Symptomatic improvement • QUALITY OF LIFE
Indwelling • Very high infection risk • High irritation and trauma risk • Professional and extra equipment usually required to change • Can work well for up to 12 weeks • Low level patient skills needed • Disliked by some users – associations with old age and infirmity • Sometimes prone to blockages
What professionals need to know • A holistic assessment of the patient must be carried out before agreeing a management plan. • ISC may only be part of an individual’s total bladder management (ACA, 2003). • Know the complicated stuff but don’t miss the obvious. • Consent
Intermittent Self Catheterisation • ISC is now much easier and safer because of new materials being available and possibly a change in our post Victorian social attitudes
Achieving success the ACA way • Patient selection • Patient discussion • General discussion • Health issues • Observations (ACA, 2003)
Intermittent • Fairly easy to use for many • Fairly low infection risk • Large amounts of supplies needed • Needs doing regularly • Allows easier sexual activity • Imitates normal bladder function
ISC Catheter Selection • Main factor is patients personal preference • Wide range of catheters currently on the market • Come in a variety of sizes ranging from 8Ch to 20Ch and are available in female or male length. • The smallest size that will drain the urine at an acceptable speed should be used.
Three main types • Those requiring a water based lubricant prior to insertion. Usually reusable. • Those needing immersion in water to activate the pre-lubricated surface. • Those lubricated and sealed ready for use from the packet.
Catheter samples • Need to carry a wide range to help to inform patient choice • Demonstrate features eg, lubrication, preparation • Use for demonstration only • Must only be used for actual catheterisation if the company takes vicarious liability
Checklist • Easy to open • Easy to handle – any special features • Low friction = low trauma • Low support for bacterial growth • Well lubricated • Good information • Smooth drainage eyes • Cost
Preparation • Try to pass urine normally • Wash hands with soap and water • Have a container ready into which you can drain the urine. (especially if it needs measuring) • Clean urethral meatus with mild soap or plain water or wash genital area from front to back • Prepare catheter; • Open packet ready to use • Lubricate if required • Soak catheter to activate lubricant • Wash hands again
Positioning • Choose a comfortable position • for men; standing, sitting or laying down if this is easiest, (penis will need to be held out from body) • For women-squatting, sitting on toilet, standing with one foot on toilet seat or lying down with knees bent • Over toilet if not using container
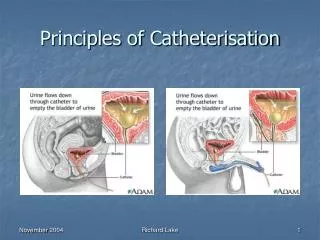
MALES • Pull back the foreskin • Hold the penis 45 degrees from body • Guide the catheter into the urethra, taking care not to touch the part of the catheter entering your body • If you experience a blockage near the bladder withdraw a little relax and try again • A small cough and push will also often get past the bladder neck • Wait until urine stops draining and slowly withdraw • Dispose of safely or store if reusable • Wash hands
FEMALES • With one hand spread the labia apart and find the urethral opening above the vagina. • A mirror can be useful initially. With practice you should be able to find the urethral opening by touch. • Slide the catheter slowly and smoothly into the urethra until urine starts to flow and drain the urine into the toilet or a container. • Wait until urine stops draining and withdraw • Dispose of safely or store if reusable • Wash hands
Frequency of ISC • Depends on the patient’s needs. • The urine passed plus residual should not total more than 500mls at each catheterisation; • Residuals over 100mls increase risk of UTIs • If patients are wet between catheterisations they may need to increase the number of times they catheterise.
Potential complications of ISC • UTI- Asymptomatic bacteriuria is common and is generally not treated unless it becomes symptomatic • If the patient experiences recurrent UTI’s their technique should be reviewed. • Blood may be present at first catheterisation - usually due to slight trauma during insertion • Pain/soreness- most patients can catheterise with minimal discomfort. On removal some experience pain or resistance, thought to be urethral spasm. Relaxing or a gentle cough can help. • Give contact details and out of hours numbers
What's all the fuss about ? • Assumption to catheterise someone inevitably means indwelling? • Frequently presented to PTs without other options considered • Doherty (2006) argues that ISC should be the first option rather than initiating an Indwelling • Despite Evidence, innovation and development Indwelling catheterisation has not diminished
Old habits die hard • There is a need develop strategies to teach the teachers to help staff identify not only weaknesses in indwelling management but be aware of competencies in ISC • Employing ISC vs Indwelling empowers pts towards self care with less clinical interventions from nurses