Download
1 / 29
290 likes | 437 Views
Discussion of four presentations on Sarcomas with complex karyotypes. JY Blay. Medical Oncology, Lyon UCBL1- CLB. GIST. Amplification 12q13-15 MDM2/CDK4. WD/DDLPS. Kinase Mutations. TSG NF1, TSC1/2. Sarcomas and locally aggressive connective tissue tumors. MPNST PEComas.

E N D
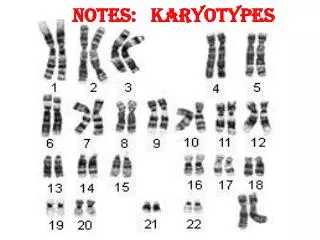
Discussion offour presentations onSarcomas with complex karyotypes JY Blay Medical Oncology, Lyon UCBL1- CLB
GIST Amplification 12q13-15 MDM2/CDK4 WD/DDLPS Kinase Mutations TSG NF1, TSC1/2 Sarcomas and locally aggressive connective tissue tumors MPNST PEComas Translocations Complex genomics SyS DFSP Ewing Mutations APC/bCat Desmoids LMS, UPS
Sarcoma subtypes Bone primary (osteosarcoma/chondrosarcoma) (8%) 8% 8% 2% GIST (18%) 2% Liposarcoma (15%) 2% 3% Soft-tissue Ewing sarcoma/pNET (4%) 3% 18% Kaposi sarcoma (3%) Dermatofibrosarcoma (5%) Unclassified sarcoma (16%) 11% Leiomyosarcoma (11%) Rhabdomyosarcoma (3%) Angiosarcoma (3%) 15% Myxofibrosarcoma (2%) 16% Synovial sarcoma (2%) 4% Endometrial stromal sarcoma (2%) 5% 3% Other very rare subtypes (8%)
Sarcomas with complex karyotypes Osteo_s Solitary_ Fibro_s MPNST Fibromyxoid_s Angio_s Ewing_s Synovial_s Rhabdomyo_s Myxofibro_s MFH Other Uterine leiomyo_s Dermatofibro_s Kaposi_s Leiomyo_s Sarcoma NOS Lipo_s GIST 0 0.2 0.4 0.6 0.8 1 1.2 1.4 Rate per 100,000
Systemic treatments Localized phase - Adjuvant CT controversial Advanced phase - Median PFS = 4-6 mos in 1st line = 2-4 mos in 2+ lines • Doxorubicin • Doxorubicin ifosfamide • Trabectedine • Pazopanib • Gemcitabine Docetaxel • Gemcitable DTIC
We need • To betterpredict relapse • To identifybetter the « driver » mutations • Biomarkers to predict for primary and secondaryresistance
4 presentations • Preclinical model • p53-/+ PTEN-/+ mice developping LMS • Theranostics • Guiding treatment of patients with NGS results • Biomarker for response • For new generation of cytotoxic treatments • CTC in sarcoma • Monitoring micrometastatic disease
A detection system for circulating tumor cells using GFP expressing telomerase-specific replication-competent adenovirus in bone and soft tissue sarcoma T. Kunisada1J. Hasei1K. Takeda1 Y. Urata3T. Fujiwara2 T. Ozaki1 1 Dept. of Orthopaedic Surgery 2 Dept. of Gastroenterological Surgery Okayama University, Okayama, Japan 3OncolysBioPharma, Inc., Tokyo, Japan
CTC in sarcoma • Predictive value in other cancers • Commercial tools imperfect for sarcoma cells • Novel technology • - detects telomerase + cells
CTC in sarcoma • 11/22 patients with detectable sarcoma cells • All histotypes (even DFSP) • Fewer CTC vs other cancer? • Predictive value? • 4/11 relapse CTC+ • 1/11 relapses CTC-
CTC in sarcoma : questions? • To be expanded and confirmed • Biological significance of CTC? • To guide adjuvant treatment? • Help to monitor response or relapse?
Identification of potential molecular biomarkers for response of soft tissue sarcoma to eribulin.Translationalresults of EORTC trial 62052 A. Wozniak*, E.A.C. Wiemer*, H. Burger, J. Allemeersch, R. van Eijsden, R.H.J. Mathijssen, S. Sleijfer, M. Smid, G.Floris, S. Marreaud,A. Nzokirantevye, R.Sciot, P. Schöffski (*equal contribution) 18th CTOS Meeting, 30/10-2/11/2013, New York, USA
Responders Non-responders Differentially expressed mRNAs (responders vs. non-responders) ALS2CR11 • amyotrophic lateral sclerosis 2 (juvenile) chromosome region, candidate 11 protein (locus 2q33.1) • Overexpressed in Leydig cells, germ cells, adipocytes • Role not known • Single reports on genomic status in cancer (mainly LOH) • In our experiment higher expression in non-responders (p=0.000102) 18th CTOS Meeting, 30/10-2/11/2013, New York, USA
Differentially expressed mRNAs and miRNAs, assessed in STS subtypes ADI – adipocytic sarcomas, LMS - leiomyosarcomas, OTH – other sarcoma subtypes;*in responders
Eribulin : questions? • mRNAs and miRNAs are differentially expressed in STS from eribulin responders and non-responders • Significance of biological pathways? • Possible predictive biomarker? • Why differences across histotypes? • Further validation studies are required • A research tool
We need • To betterpredict relapse • To identifybetter the « driver » mutations • Biomarkers to predict for primary and secondaryresistance
What is a good target? Expression Possible target Expression + activation Promising target Expression + activation + mechanism A major target Expression + activation + mechanism + drug Clinical trial
Dual PTEN/P53 suppression promotes high grade sarcomas by activating Notch Eva Hernando, Ph.D.
Dual PTEN/TP53 suppression and sarcomagenesis • Mutational profling of sarcoma patients • Dual suppression in SMC • P53-/+ & PTEN -/+ • HGUPS, LMS • Activation of the Notch pathway, and sensitivity to GSI
Gamma-secretase inhibition suppresses the clonogenic and invasive potential of tumor cells
Sarcomagenesis: questions • A relevant model for LMS/UPS subsets? • Screen human tumors • To reevaluate the role of GSI/Notch pathway modulators in vivo in the clinics?
NGS analysis • N=57 patients, • Druggable alterations • Documented responses • Documented SD
NGS analysis • N=57 patients, • Documented responses • Documented SD • Value of GMI? • PFS2/PFS1 • Denominator? • From N of 1 to prospective series with homogenous molecular diagnosis
Theranostics : questions • Valuable strategy • N of 1 trials methodology • Guide research programs in larger patients sets • Negative results also should be informative • Difficult analysis when combinations are used
Conclusions • Four important reports • Biomarkers and predictive factors for relapse and resistance are needed. • Preclinical models to guide us for drug development. • Translational research : biopsy and rebiopsy
A World Sarcoma Network is needed Join us! 9/2/2014 28
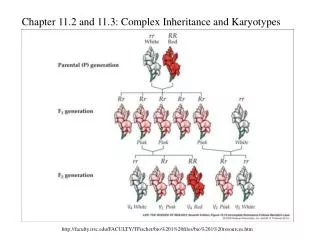
Connective tissue tumours5 types of sarcomas • Specific translocations generating fusion genes 15% • Kinase mutations (KIT…) 15% • Gene inactivation (NF1…) 10% (?) • Amplifications chromosome 12 (MDM2+CDK4) 15% • Complex genetic alterations (MFH, LMS, ...) 50%