Download
1 / 67
680 likes | 732 Views
General Anaesthesia & Sedation for Dental Procedures. Dr Walid Zuabi Consultant Anesthetist FCA RCSI. Anaesthesia. Terminology: An- No Esthesia Sensation. Sensations. Peripheral: Pain Temperature Touch deep light Proprioception Special senses

E N D
General Anaesthesia & Sedation for Dental Procedures Dr Walid Zuabi Consultant Anesthetist FCA RCSI
Anaesthesia • Terminology: • An- No • Esthesia Sensation
Sensations • Peripheral: • Pain • Temperature • Touch • deep • light • Proprioception • Special senses • Central: Awareness: Apprehension; Fear and Anxiety
Anaesthesia Implies reversibly rendering the patient unconscious by drugs for the execution of a painful operative procedure - in a titrated & controlled way.
Surgery • Trauma stress • Metabolic Response to stress: • Neural Component Autonomic system - Sympathetic - Parasympathetic • Endocrine Component Hormonal System - Growth Hormone - Cortisol - glucagon - Antidiuretic - Renin & Aldosterone
Anaesthesia • Modulates the stress response by blocking the afferent limb of the response • Pain and awareness are blocked by anaesthetic drugs but other afferent limb factors are not/ Hypovolemia & hypoxemia Complete medical management of the patient: pre, intra & post-op management.
Anaesthesia • Modern Anaesthesia is Composed of: • Hypnosis: Controlled Loss of Awareness • Analgesia: Loss of Pain • (+/-) Muscle Relaxation( Controlled muscle Paralysis)
Hypnosis *Hypnosis: The state of being asleep. • Pharmacologically induced: non-physiological very deep level of sleep that deprives the patient from his control. • Can and should be titrated according to the level of surgical stimulus
Analgesia * State of freedom from pain Analgesia vs. anaesthesia: • Analgesia can be brought about by local or regional techniques, or drugs with specific pain receptors action ( Opioids) without Loss of consciousness.
Muscle Relaxation • Paralyzing the patient’s skeletal muscles by use of drugs that block the ACH receptors at the Neuromuscular junction • Purposes: • Facilitate airway management • Prevents aspiration • Control of Ventilation • Facilitate Surgery • Patients to be artificially ventilated.
Stages of Anesthesia 1- Stage of analgesia: Diminished pain perception, verbal contact maintained laryngopharyngeal reflexes and present voluntary control. 2-Stage of uninhibited response/ Excitement Consciousness lost, verbal contact and voluntary control lost uncontrolled, exaggerated, withdrawal type response to any stimulus Protective laryngopharyngeal reflexes maintained! 3- Stage of Surgical Anaesthesia: 4- Stage of Respiratory Arrest
In Dentistry 1- Local Anaesthesia 2- General Anaesthesia 3- Sedation
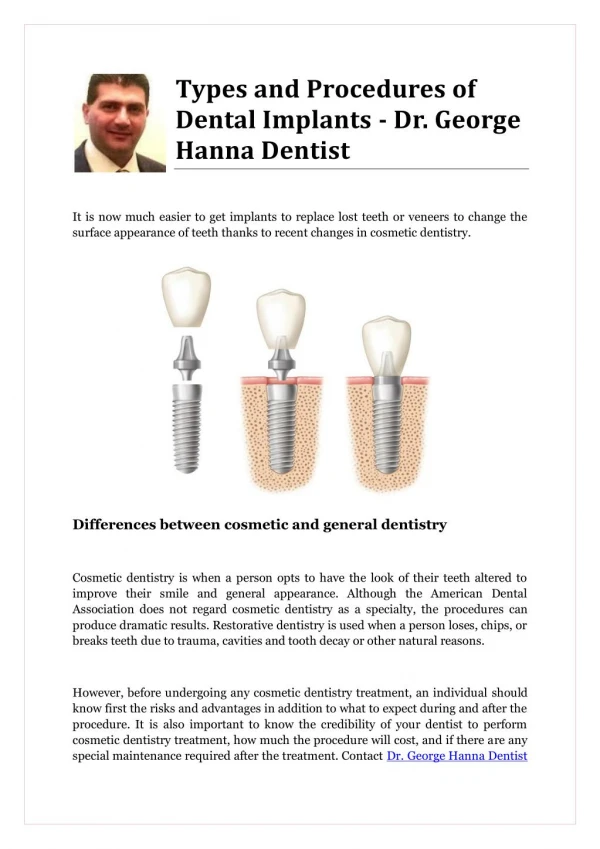
Dental Procedures Requiring General Anesthesia 1- Oral Surgery: Removal of impacted teeth Insertion of implants 2- Restorative Dentistry: 3- TMJ: Arthroscopy & Arthroplasty 4-Maxillofacial Surgery: Trauma, Tumors or reconstructive 5- Special patient groups: • Young Children with systemic Diseases (hemophilia & CHD) • Patients with poor controlled Seizures - Those with an oral septic focus
Summary of Fasting Recommendations Clear liquids 2 Hrs
Summary of Fasting Recommendations Clear liquids 2 Hrs Solids 6 Hrs
Summary of Fasting Recommendations Clear liquids 2 Hrs Solids 6 Hrs Nonhuman milk 6 Hrs
Summary of Fasting Recommendations Clear liquids 2 Hrs Solids 6 Hrs Nonhuman milk 6 Hrs Infant formula 6 Hrs
Summary of Fasting Recommendations Clear liquids 2 Hrs Solids 6 Hrs Nonhuman milk 6 Hrs Infant formula 6 Hrs Light meal 6 Hrs
Summary of Fasting Recommendations Clear liquids 2 Hrs Solids 6 Hrs Nonhuman milk 6 Hrs Infant formula 6 Hrs Light meal 6 Hrs Breast milk 4 Hrs
Preoperative Pharmacologic Interventions • GI stimulants (metoclopramide) • Block of gastric acid secretion • H2 antagonists (cimetidine, ranitidine) • PPI (omeprazole, lansoprazole) • Antacids (sodium citrate) • Antiemetics (ondansetron) • Anticholinergics (atropine, glycopyrrolate)
Problems Related to Dental Anaesthesia 1- In & Outpatient selectivity 2- Competition for the Airway by both Dentist and Anaesthetist 3- Patients are often young 4- Special needs’ patients
Conduct of Anaesthesia Pre-Operative Assessment Intra-Operative Management Post-Operative Care
Pre-Operative Assessment - History: medical, surgical, anaesthetic & Allergy - Physical Examination - Investigations: accordingly.. INR or ECHO! - Informed Consent: signed by patient or guardian
Patient selection • Only ASA I and ASA II groups should undergo dental sedation in a general dental practice (clinic).
Intra-Op Management 1- Establishing Monitoring: Heart Rate, Blood Pressure, Electrocardiogram, Pulse Ox & ETCO2 2- Induction of Anesthesia : Hypnosis => - Intravenous Drugs: (e.g. Sodium Thiopentone , Propofol, Etomidate, Ketamine Analgesia => - Nitrous Oxide gas - Opioid Drugs: Morphine, Pethidine, Fentanyl, Alfentanyl, Sufentanyl, Remifentanyl Muscle Relaxation => - Short Acting: Suxamethonium - Intermediate: Atracurium, Cisatracurium, Vecuronium, Rocuronium, - Long Acting: d-tudocurarine, Pancuronium
Intraoperative Management continued 3- Maintenance of Anaesthesia => - IV infusion for short acting drugs - Inhalational Agents for Hypnosis: (e.g. Halthane, Sevoflurane, Isoflurane , Enflurane, etc ) - Intermittent doses for intermediate or long acting muscle relaxants and analgesics
Intraoperative Management continued 4-Securing the Airway : * Using a Cuffed Endotracheal Tube - Orally - Nasally for surgical access * Throat pack * Meticulous Suctioning
Intraoperative Management continued 5- Securing Ventilation - Spontaneous Breathing - Manual ventilation - Ventilator/ PPV 6- Surgery Starts * Continuous Monitoring for - A,B,C - Adequate Anaesthesia -Necessary management
Intra-operative Issues • Loose Teeth • Surgical Debris • Bleeding • Secretions • Use of Throat Pack • Endocarditis Prophylaxis
Postop Management 1- Emergence from Anesthesia * Anaesthetics off Recovery in Lateral Position ** Reversal of residual Muscle relaxation Anti-dote: Neostigmine withatropine * Extubation 2-PACU: Monitoring and Active Management 3- Assessment before Discharge By anaesthetist
Sedation • Definition: A state of controlled depression of consciousness that allows patients to tolerate unpleasant procedures while maintaining adequate cardio-respiratory function and the ability to respond purposefully to verbal command and/or tactile stimulation.
Aim of Sedation • Achieving anxiolysis and patient cooperation
Which patient groups ? • Dental Anxiety & Phobia. • Prolonged traumatic procedures. • Medical conditions aggrevated by stress. • Patient cooperation. • Special needs. • Children and young adults • Anxious adults
DRUGS USED 1- Benzodiazepines 2- Neuroleptanalgesia 3- Nitrous Oxide 4- Sedative Anaesthetics ( I.V. Hypnotic drugs)
Benzodiazepines • Most widely used. • Wide safety Margin. • IV & Oral formulations available.
Benzodiazepines Functions 1- Anxiolytic 2- Sedative (hypnosis) sleep promotion 3- Amnesia/ RETROGRADE 4- Central muscle relaxant effect 5- Anticonvulsant
Benzodiazepines • Diazepam Oral: 2 mg q 8 hrs for anxiety 10-15 mg for premedication 2 hrs pre-op (in Hospital) • IV or IM. painful on injection Diazemulus(lipid emulsion): painless on injection 5 mg/ml
Benzodiazepines Diazepam(Continued) • Good anxiolytic • Poor amnesic • Minimal CV depression • Long Duration of action • Active metabolites
Benzodiazepines Midazolam • Indications: - Conscious sedation - Co-induction of GA Doses: - For pre-op sedation 0.07 – 0.08 mg/kg 1 hr before procedure I.M injection - Individualized dose I.V
Benzodiazepines Midazolam • Best amnesic , good hypnotic • Some CV depression • Readily produces general anesthesia • Duration < 2 Hrs
Benzodiazepines Temazepam • Only Oral. • Doses : - Insomnia : 10 – 30 mg - Premedication: 10 – 20 mg 2 HrsPreop • Good Hypnotic • Short duration • May cause dysphoric reactions in young adults
Benzodiazepines • Antidote: Flumazenil(Anexate) • A specific antagonist • I.V • Essential requirement if Benzodiazepines are used. • 0.2 mg IV every 15 seconds • Rapid recovery • Duration: 15 min • Re-sedation if long acting BZD is used • Can precipitate withdrawal reaction in habituated patients.
Neuroleptanalgesia • Major tranquilizers: chlorpromazine, droperidol & • Opiates: Fentanyl, morphine & Codeine ============================= • Many side effects - Behavioral syndromes: - inhibition of purposeful movement - inhibition of learned behavior - catalepsy: a condition characterized by rigidity of extremities and decreased sensitivity to pain