Download
1 / 29
310 likes | 809 Views
Assessment of Heart and Great Vessels. Christine M. Wilson Viterbo University. Objectives. Landmarks Structures Cardiac cycle Developmental/transcultural Risk factors Subjective data Objective data. Position in the Chest.

E N D
Assessment of Heart and Great Vessels Christine M. Wilson Viterbo University
Objectives • Landmarks • Structures • Cardiac cycle • Developmental/transcultural • Risk factors • Subjective data • Objective data
Position in the Chest • Beneath precordium—area on anterior chest overlying the heart and great vessels • Located in mediastinum—middle third of chest—between the lungs
Heart is an upside down triangle in the chest • Top of heart is Base, bottom is Apex
Extends from 2nd to 5th ICS and from Rt sternal border to Lt MCL • Great vessels above base of heart
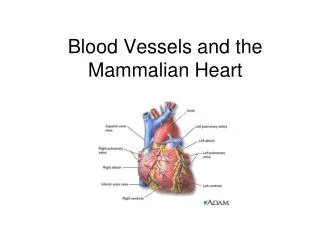
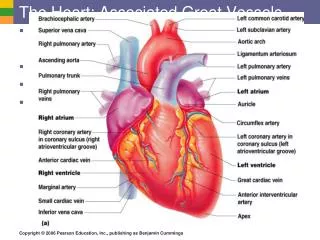
Blood Flow • Inferior vena cava • Right atrium • Right ventricle • Pulmonary artery • Pulmonary vein • Left atrium • Left ventricle • Aorta
Tricuspid valve: right AV Mitral valve: left AV Pulmonic Valve: right Aortic Valve: left It is the closure of the heart valves that we hear as heart sounds. Valves of the Heart
Diastole Tricuspid/mitral valves open Ventricles relax and fill with blood Ventricular pressures increases Tricuspid/mitral valves close causing first heart sound S1 LUB dub Systole Ventricular contraction increases pressure Pulmonic/aortic valves open; blood ejects Ventricular pressure drops Pulmonic/aortic valves close causing second heart sound S2 lub DUB Cardiac Cycle
More heart sounds • Events of right heart occur slightly later • S1 Mitral valve closes then tricuspid • S2 Aortic valve closes then pulmonic • Sound radiates with direction of blood flow • S1 heard loudest at apex • S2 heard loudest at base • Murmurs—turbulent flow through chambers and valves • Swooshing, blowing sound
Pumping ability • Right side pumps blood to lungs • Left side pumps blood to body • Cardiac output—volume of blood pumped per minute • dependent upon volume ejected per stroke and heart rate (CO=SV x rate) • Normal cardiac output 4-6 L per minute
Carotid arteries Central arteries branching from aorta Jugular veins Internal and external Empty into superior vena cava Great Vessels—Neck
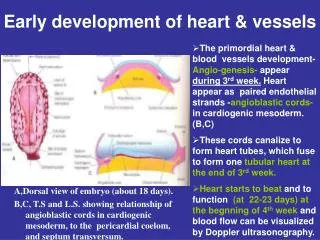
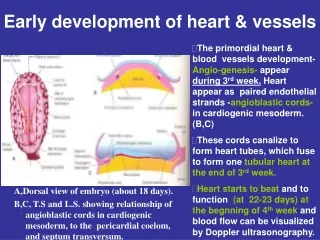
Developmental Considerations Fetal • Fetal heart begins to beat at 3 weeks • Oxygenation takes place through the placenta • Blood returned to the Right side of the heart and bypasses lungs • Foramen ovale-opening between atrium • Ductus arteriosus-opening b/tw PA and Aorta
Changes take place at birth! • Blood is oxygenated through lungs • Foramen ovale closes in one hour • Ductus Arteriosus closes in 10-15 hours • Left ventricle pumps blood to entire body; by one year, left ventricle twice as large as the right
Pregnant Female • Blood volume increases by 30-40%, mostly during the 2nd trimester • Increases Stroke Volume and CO • Rate increases by 10-15 BPM
Aging Adult • Cardiac aging depends on lifestyle factors • Stiffening of large arteries due to calcification of vessel walls causes increased workload for heart • BP increases by 25-30% • LV wall thickness increases by 25%
Aging Adult (con’t) • Arrhymias increase with age • Conduction changes are common • 50% of deaths in elderly due to cardiovascular disease • Hypertension increases with age • Systolic greater than 140 and Diastolic greater than 90 • Heart failure common
Transcultural Considerations Heart Disease and Stroke • 1/3 of deaths from culturally diverse backgrounds • Prevalence higher in blacks, followed by whites, then Mexican Americans • Native Americans (<35) CAD 2X greater than other groups • Black males 2X more likely to die from stroke as white males
Transcultural Considerations Heart Disease and Stroke (con’t) • Blacks 20-40 years • Increased # of deaths from CVD compared to whites • Increased mortality in black females over black males • Black and Mexican American females higher CVD risk factors
Risk Factors for Heart Disease, Stroke, and Hypertension • Smoking • Increased cholesterol levels (LDL) • Obesity • Diabetes • Oral contraceptives • Post-menopause
Chest Pain Dyspnea Orthopnea Cough Fatigue Cyanosis or pallor Edema Nocturia Past cardiac history Family cardiac history Cardiac risk factors Subjective Data
Objective Assessment Order of the exam • Pulse and blood pressure • Extremities:Peripheral Vascular System • Neck Vessels • Precordium
The Neck Vessels Carotid arteries • Palpate • Individually, with gentle touch • Auscultate • Angle of jaw, mid-cervical, base of neck • Patient to exhale and hold breath
The Precordium • Inspect for pulsations • Palpate the apical pulse • 5th ICS MCL • “Bump” of the left ventricle against chest wall during systole • Palpate apex, Lt sternal border, base • Percussion not usually done
Auscultation Areas to listen • Aortic valve area: 2nd Rt. intercostal space • Pulmonic area: 2nd Lt. intercostal space • Erb’s Point: 3rd Lt. intercostal space • Tricuspid area: 5th Lt. intercostal space • Mitral area: 5th intercostal space at MCL
Ascultation tips • Concentrate • Inch diaphragm in Z pattern, base to apex • Aortic—pulmonic—Erb’s—tricuspid—mitral • Listen to one sound at a time • Rate • Rhythm • Identify and assess S1 and S2 separately • Listen for extra sounds
S1 is louder than S2 at Apex. S2 is louder than S1 at Base. S1 coincides with the Carotid artery pulse Visualize what’s under the skin REMEMBER