Download
1 / 24
260 likes | 504 Views
Vertebral PTA: Indications and Technique. Patrick L. Whitlow, MD Director, Interventional Cardiology The Cleveland Clinic Foundation. I have NO relationships related to this presentation. Off label use of products will be discussed in this presentation. .

E N D
Vertebral PTA:Indications and Technique Patrick L. Whitlow, MD Director, Interventional Cardiology The Cleveland Clinic Foundation I have NO relationships related to this presentation.Off label use of products will be discussed in this presentation.
Vertebral Artery Stenosis/Occlusion: Symptoms • 50% present with stroke as 1st symptom • Embolic: sudden maximum onset, blurred vision, or homonymous hemianopsia- usually originate from VA origin • Vertebrobasilar TIA’s - 22-35% stroke by 5yrs, and mortality with CVA 20-30%
Vertebral Artery Stenosis/Occlusion: Symptoms • Hemodynamic: tandem/severe lesions Multiple Symptoms: vertigo,nausea, visual dysfunction; perioral paresthesia; ataxia; dysarthria; syncope; headache; nystagmus; facial palsy,numbness • Thrombotic: prolonged, fluctuating course to maximum neurologic deficit or coma
Vertebral Artery Stenosis/Occlusion: Symptoms • Symptoms: Hemodynamic Thrombotic • Predominantly occur in Patients with Multi-Vessel Disease because of Redundant Blood Supply • Emboli may occur with isolated disease
Vertebral Artery Stenosis/Occlusion: Treatment Symptomatic angiography > revascularization Asymptomatic majority get medical rx Consider revascularization if high risk for CVA (Remember 50% of these have no warning TIA’s) > 70% stenosis, esp. if worsening and dominant or single vertebral Posterior hypoperfusion or decreased reserve
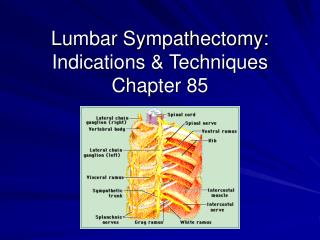
Vertebral Artery Stenosis/ Occlusion: Treatment Traditional: Avoid Hypotension;use Antiplatelet or Anticoagulant; carotid duplex; IC Doppler Vertebral Origin Lesions difficult to quantify w/o angiography, and need to assess collaterals >Consider surgery for V1 disease(unusual) >Consider percutaneous intervention
Background • Limited data exists on percutaneous treatment of symptomatic vertebral artery disease • Surgical treatment for symptomatic vertebral artery disease has significant morbidity and is limited to V1 segment
4 3 2 1
Vertebral Artery Disease:Surgery for V1 Segment • Carotid-Vertebral Transpositionor Endarterectomy • Mortality > 4% • Morbidity 10-20%
Vertebral Surgery Complications of V1 Surgery: Transient ischemic attack 2.2% Thrombosis 8.7% Koskas,Ann Vasc Surg 9:515-524 Recurrent laryngeal nerve palsy 2% Horner’s syndrome 15% Lymphocele 4% Chylothorax 0.5% Thrombosis 1% Beurger, Long Term Results in Vascular Surgery 1993:69-79
Vertebral Artery Stenosis / Occlusion: Treatment • No randomized studies Meds vs Surgery and No Trials Intervention vs either Meds or Surgery • Symptoms are frequently vague: may need flow study to determine significance Neuro Consult very helpful
Vertebral Artery Angiography Baseline Angiography: 30-45% LAO Arch Angio with 4 vessel study to define collateral support of the posterior circulation( non-selective) For Selective vertebral: JR4,Berenstein , MP A-P ; 20-30o contralateral oblique;cranial 20º
Vertebral Artery Stenting • Pretreat with ASA, Clopidogrel > 3 days • Access Femoral Artery, or Radial / Brachial • JR4, IMA, MP, H1, 6Fr Guide or /Ansel Sheath • Heparin 50-70 units/kg: ACT 240-300 seconds • Rarely consider IIb/IIIa blocker (IC Hemorrhage) • Consider Embolic Protection: Tortuosity, landing zone, branches, retrieval
Vertebral Artery Stenting • Consider subclavian “Buddy-Wire” • Roadmap; cross with 0.014” wire or EPD - stay out of Branches • Consider predilation with coronary balloonvs direct stent • Artery size 2.7 - 5.5mm, mean 4.5mm; lesion length typically 5-10mm - so use coronary stents
Vertebral Artery Stenting • If ostial, use balloon expandable stent for precise placement ~2mm into subclavian origin • High restenosis rates in some series(up to 43%) - ?ostial coverage, ?recoil • Consider DES; stents with radial force
Vertebral Artery Stenting • Precise Deployment, slow inflation to ~8atm • Pull balloon back high pressure (12-14atm) to minimize risk distal dissection, Flare edge • Nitro and angio to assess size, edges
Vertebral Artery Stenting • Optimize stent size with post-dilation • Frequent Neuro status checks • Final angios to asses for embolization, EPD damage ,wire trauma,kinking • Esp with EPD, push/pull guide into stent for retrieval
Vertebral Artery Stenting • Usual post Sheath care • Usual ASA, Plavix • Independent Neuro Exam • Monitor overnight • Usual Risk Factor Control
Vertebral Artery Stenting Results • 94-100% Technical Success • Complications: Dissection, spasm, embolism, CVA, TIA, thrombosis, IC bleeding - All rare • Usual 1-2% sheath related events
Vertebral Artery StentingFollow-Up • Work with a Neurologist • Non-invasive assessment not reliable • Consider Re-Angio 4-6 months • Restenosis 10-43% - usually asymptomatic • Randomized Trials, long term follow-up are needed!! ?Role of EPD, DES, surgery
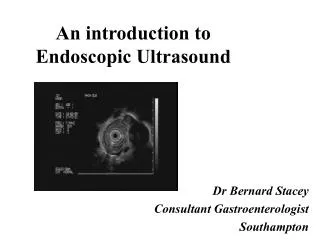
Severe Ostial Vertebral Stenosis Post-procedure Pre-procedure