Download
1 / 27
270 likes | 448 Views
Leveraging Technology to Improve Population Health in an PCP Driven Accountable Care Organization. July 30, 2013. Curtis P. Page, MD CEO & President Commonwealth Primary Care ACO Chris Connor Vice President-Central Alere Accountable Care Solutions.

E N D
Leveraging Technology to Improve Population Health in an PCP Driven Accountable Care Organization July 30, 2013
Curtis P. Page, MDCEO & President Commonwealth Primary Care ACOChris ConnorVice President-CentralAlere Accountable Care Solutions
Why? • SYSTEMIC and BEHAVIORAL • The U.S. health system is highly fragmented, with limited public health and primary care resources and a large uninsured population • he United States has a relatively weak foundation for primary care and a shortage of family physicians (American Academy of Family Physicians, 2009; Grumbach et al., 2009; Macinko et al., 2007; Sandy et al., 2009) • Many Americans rely on emergency departments for acute, chronic, and even preventive care (Institute of Medicine, 2007a; Schoen et al., 2009b, 2011). • The United States stands out from many other countries in not offering universal health insurance coverage. • Cost sharing is common in the United States, and high out-of-pocket expenses make health care services, pharmaceuticals, and medical supplies increasingly unaffordable (Commonwealth Fund Commission on a High Performance System, 2011; Karaca-Mandic et al., 2012). • Health insurance premiums are consuming an increasing proportion of U.S. household income (Commonwealth Fund Commission on a High Performance System, 2011).
Herein lies the #1 Problem • YOU GET WHAT YOU PAY FOR!!! • It’s just the business model • #1 Problem with US healthcare: Fee for Service (FFS) • Reimbursement & 3rd Party Payorpolicies • Humans are simple creatures: We do what we get paid to do. • We do not do a lot of what we do not get paid to do. • Epidemic of doing more things that we get paid to do: • Creates overutilization; “55% of US patients do not receive • appropriate care”, Deloite 2012 • US 3rd party payor system pays for episodic care with a emphasis on procedures. Underpayment for more complex intuitive care. Poor payment for prevention, care coordination and certainly does not pay for outcomes. • We get paid for illness and not for healthand wellness • Best Characteristic of US healthcare: We do not provide the healthcare that is NEEDED. We provide all of the healthcare that is POSSIBLE. • Any reasonable attempt to rein in costs has to be fundamentally based on changing the reimbursement system. • Pay for Quality to Pay for Performance to Full Capitation (Risk) • When providers are paid for outcomes they begin to think creatively and meaningfully about the total care of the patient.
Other issues • Historical Laws that have dissuaded physician collaboration • Stark • Anti-Trust • Anti-kick Back • Collective Bargaining • Meant to dissuade behavior that could drive up market prices, but the result is that it has given significant power and control over healthcare to non-physicians: commercial payors and hospital. • End result is fragmented healthcare and near complete lack of physician socialization or collaboration. • Explains the necessity of both clinical and financial integration. Without financial relationships there can exist no driver for clinical collaboration.
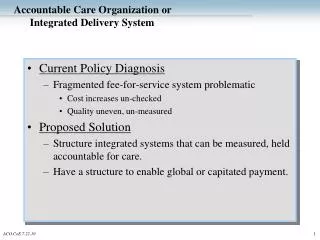
ACO Business Model The ACO Profits by lowering expenditures compared to other physicians
Business Model: Medicare and Commercial Opportunities Value-based contracting opportunity extends across all lines of business Medicare Our Current Benchmark: Approximately 50 Million US Dollars (5,500 Lives) Modest 10% savings: $ 5,000,000 Savings split 50/50 with CMS: $2.5 Million to Commonwealth ACO Commercial Major Payor #1Attribution: 5,400 Lives Major Payor #2 Attribution: 4,500 Lives Etc, etc Potential profits in the millions. Each panel of 200 patients has the potential to generate about $100,000 per year (Medicare) and $50,000 (Commercial) in “gain share” revenue.
The ACO as business model Start with the premise that in the current state US HEALTHCARE DOES NOT WORK Underlying Theme: Change. We must do something different in order to have the possibility of achieving something different. ASSUMPTION: If you are not a part of the solution Continue to practice today as you always have ASSUMPTION (Cont.): YOU ARE PART OF THE PROBLEM
Question • How do you get from point A to point B? • You create what does not exist. • You manage what is not managed. • The economic opportunity is tremendous because you are carving out a niche that is currently needed and devoid. • Recognition and action by providers is the key. This is not a passive process.
The ACO Opportunity: Build, Joint Venture or Foster Business Relationships to support use and development of the “Medical Middle” SNF Patient’s Home Hospital ER Inpatient Hospital LTAC Lab PCP Office Specialists Office Home Health Urgent Care Hospitalists Ambulatory Surgery Center Retail Clinic Hospice Own Outright Outpatient Procedure Center Physical Therapy Financial Partner Clinical Partner Only Radiology Unknown; Potential Ownership vs Financial Partner Specialty Hospital
The ACO Opportunity: Build, Joint Venture or Foster Business Relationship to support use and development of the Medical Middle SNF Patient’s Home Hospital ER High Cost High Cost High Cost Inpatient Hospital LTAC Physician’s Office High Cost High Cost Home Health Urgent Care High Cost Retail Clinics Hospice
Keys to success • Must have long term goals in place • Systematic approach to utilization and disease management • Providing the right care at the right place at the right time • Minimal influence by potential “cost centers” • Hospitals • Specialist • Infrastructure Investment • Self Management Education • Advanced Nurse Care Management (Case Management & Clinical Nursing) • Information Technology & Communication Systems • Practice level training to deliver value • Moving from a Culture of Me to a Culture of We • Follow protocols and process chosen by organization • Use and influence chosen network • Reward specific patient and physician behaviors that support collaboration
Communication • Single most important key to success is communication: • Communication amongst PCPs to develop standards methodologies • and care pathways • Communication between PCPs and Patients that improves care • Written care plans • Patient portals • Care reminders • Participation in Accountable Care Organization care pathways • and utilizing ACO Network • Communication between Hospitalists and PCPs Practices • Communication systems that accumulate health and utilization data • and deliver actionable messages to caregivers (Analytics). • Accumulation of utilization data for feedback to PCPs to influence • practice patterns and network utilization patterns • Communication between ancillary providers (SNF, HH, LTAC, Rads, Lab, • Specialists, Hospitals, ASC’s, UC, Retail Clinics)and PCP practices
Technology to Leverage • Caregiver to Caregiver systems of communication • HIPPA Compliant • Based on text messaging and emailing • Cortext by Imprivata • Health Information Exchange • Real Time Data • Ability to engage several stakeholders on one cloud based system • Data Analytics Systems • Propriety data analysis • Point-of-Care Decision Support Tools • In Home Monitoring Solutions
PCP Oversight PCP Care Coordinators monitor patient compliance and goals PCPs and ACO monitor all outside costs Specialist Care Nurse Coordinator Patient Home Devices Home devices used for higher-acuity participants in our Heart Failure, Diabetes and Chronic Obstructive Pulmonary Disease (COPD) programs. It is hooked up to separate devices used to measure or monitor symptoms relevant to the condition, including weight scales for heart failure and glucometers for diabetes.
Strategies for Success • Manage “episodic costs” (70% of costs) through intensive Nurse-based Care Coordination • Using evidence-based medicine guidelines available at point of care (Milliman Guidelines) • “Right care, right setting, right cost” • Apply analytics to identify cost and quality opportunities and patients in greatest need • Maximize on quality scores by constantly monitoring population health and outcomes • Provider selection • Only work with efficient specialists, hospitals and ancillary • Patient support of chronic conditions and risk factors • Empower patient to self-manage, improve compliance and improve quality metrics • Home monitoring programs when appropriate
Analytics to Focus Population based Performance • Every population is unique – assess history to determine opportunity and monitor performance based on key metrics
Individualized Care Plans • Focused on to 10% at greatest risk • Analytics tools create opportunities for intervention
Real-Time Decision Support & Population Analytics • Total Populations • Episode Grouping Analytics & Decision Support enable endless opportunities to better manage our patients and our costs • Predictive Modeling • Intelligent Order Sets • Quality Measures • Risk Stratification • Predictive Modeling • Medication Management • Patient Engagement & Education • Patient & Population Health Management • Disease Registries • Meaningful Use Stage 2
Health Information Exchange Health Information Exchange (HIE) creates a virtual community where clinicians can access the most up-to-date patient information and better coordinate care and treatment. • CommonweatlhHealth Information Exchange (HIE) extracts clinical information from several different repositories and integrates that data within a single longitudinal health record that all care providers can securely access. • Our HIE captures data from patients, doctors, payers, and devices, integrating it in one patient health record (PHR). • HIE will connect our entire healthcare network.
Biometric & Diagnostic Devices • Whether at the point of care or in the home, data should be actionable, comprehensive and increasingly accessible to patients, physicians, and payers. • Moving testing closer to the individual closes crucial gaps in time, provides greater visibility, and accelerates decisions that lead to better outcomes. • Familiar biomarkers, small sample sizes, and are easy-to-use. • Real-time connections transmit results to HIE • Monitor treatment compliance and intervene earlier. Reduce the risk of serious events and healthcare costs. • Devices for the most costly chronic conditions: Congestive Heart Failure, COPD, Anticoagulation, Diabetes.
Data Collection & Storage • Getting ALL the data is imperative to full visibility of patient care/costs • Accumulating the data is a marathon, not a sprint • Must be zero to minimal change to physician workflow • Must provide value to the physician at the point of care • Patient/Entity identification is key to accurate cost measurement • Need to have master indexing system to prevent misidentification • Cloud based secure storage allows 24/7 access and required HIPAA security
Data Collection & Storage Physician EHR Data must flow from and to the points of care through the HIE Care Monitor Hospital EHR Ancillary Providers HIE Data Analytics Single, consolidated view of patient with actionable data at the point of care Clinical Decision Support Home Monitoring
Summary • US Healthcare is of Poor Value • Due to FFS payment system. • Poor primary care base • Disconnected Care • Solution depends on Changing Physician and Patient Behavior • Behavior changes depend on: • PCP engagement • Deployment of meaningful communication systems • Practice-embedded resources (care management, case management, • self management education, etc) to create better outcomes • Utilization of new and improved resources and processes within the • previously neglected “medical middle” • dependent on aligning incentives and reforms to the • reimbursement system
Commonwealth Primary Care ACOGreater Phoenix Integrated Practice Affiliationinfo@gpipa.com480-296-1276For Primary Care, By Primary Care
The Changing Landscape of Reimbursement Increasing Provider Risk GLOBAL CAPITATION / BUNDLED PAYMENT DOWNSIDE RISK SHARING “Shared Risk” UPSIDE GAIN SHARING “Shared Savings” PAY FOR “Clinical” PERFORMANCE (P4P) FEE FOR SERVICE