Download
1 / 1
10 likes | 180 Views
Development of a video-based cataract surgery assessment tool for use in ophthalmology residency Asim V. Farooq, BA 1 , Omar Krad, MD 2 , Susanne Tidow-Kebritchi, MD 2 , Charles Bouchard, MD 2

E N D
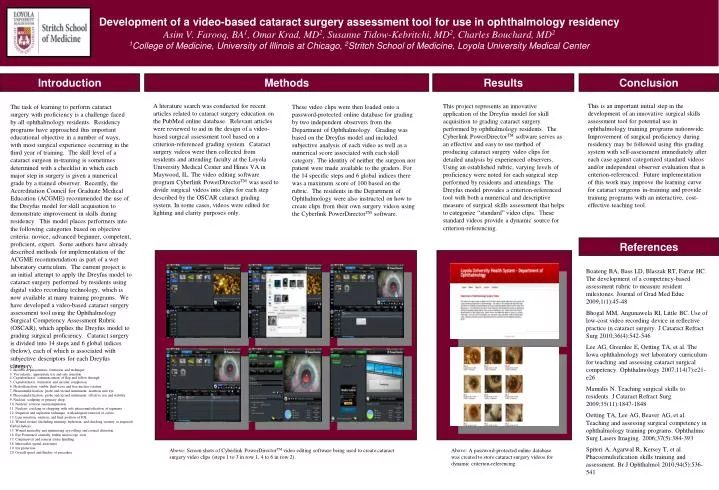
Development of a video-based cataract surgery assessment tool for use in ophthalmology residency Asim V. Farooq, BA1, Omar Krad, MD2, Susanne Tidow-Kebritchi, MD2, Charles Bouchard, MD2 1College of Medicine, University of Illinois at Chicago, 2Stritch School of Medicine, Loyola University Medical Center Introduction Methods Results Conclusion A literature search was conducted for recent articles related to cataract surgery education on the PubMed online database. Relevant articles were reviewed to aid in the design of a video-based surgical assessment tool based on a criterion-referenced grading system. Cataract surgery videos were then collected from residents and attending faculty at the Loyola University Medical Center and Hines VA in Maywood, IL. The video editing software program Cyberlink PowerDirectorTM was used to divide surgical videos into clips for each step described by the OSCAR cataract grading system. In some cases, videos were edited for lighting and clarity purposes only. This is an important initial step in the development of an innovative surgical skills assessment tool for potential use in ophthalmology training programs nationwide. Improvement of surgical proficiency during residency may be followed using this grading system with self-assessment immediately after each case against categorized standard videos and/or independent observer evaluation that is criterion-referenced. Future implementation of this work may improve the learning curve for cataract surgeons in-training and provide training programs with an interactive, cost-effective teaching tool. This project represents an innovative application of the Dreyfus model for skill acquisition to grading cataract surgery performed by ophthalmology residents. The Cyberlink PowerDirectorTM software serves as an effective and easy to use method of producing cataract surgery video clips for detailed analysis by experienced observers. Using an established rubric, varying levels of proficiency were noted for each surgical step performed by residents and attendings. The Dreyfus model provides a criterion-referenced tool with both a numerical and descriptive measure of surgical skills assessment that helps to categorize “standard” video clips. These standard videos provide a dynamic source for criterion-referencing. The task of learning to perform cataract surgery with proficiency is a challenge faced by all ophthalmology residents. Residency programs have approached this important educational objective in a number of ways, with most surgical experience occurring in the third year of training. The skill level of a cataract surgeon in-training is sometimes determined with a checklist in which each major step in surgery is given a numerical grade by a trained observer. Recently, the Accreditation Council for Graduate Medical Education (ACGME) recommended the use of the Dreyfus model for skill acquisition to demonstrate improvement in skills during residency. This model places performers into the following categories based on objective criteria: novice, advanced beginner, competent, proficient, expert. Some authors have already described methods for implementation of the ACGME recommendation as part of a wet laboratory curriculum. The current project is an initial attempt to apply the Dreyfus model to cataract surgery performed by residents using digital video recording technology, which is now available at many training programs. We have developed a video-based cataract surgery assessment tool using the Ophthalmology Surgical Competency Assessment Rubric (OSCAR), which applies the Dreyfus model to grading surgical proficiency. Cataract surgery is divided into 14 steps and 6 global indices (below), each of which is associated with subjective descriptors for each Dreyfus category. These video clips were then loaded onto a password-protected online database for grading by two independent observers from the Department of Ophthalmology. Grading was based on the Dreyfus model and included subjective analysis of each video as well as a numerical score associated with each skill category. The identity of neither the surgeon nor patient were made available to the graders. For the 14 specific steps and 6 global indices there was a maximum score of 100 based on the rubric. The residents in the Department of Ophthalmology were also instructed on how to create clips from their own surgery videos using the Cyberlink PowerDirectorTM software. References Boateng BA, Bass LD, Blaszak RT, Farrar HC. The development of a competency-based assessment rubric to measure resident milestones. Journal of Grad Med Educ 2009;1(1):45-48 Bhogal MM, Angunawela RI, Little BC. Use of low-cost video recording device in reflective practice in cataract surgery. J Cataract Refract Surg 2010;36(4):542-546 Lee AG, Greenlee E, Oetting TA, et al. The Iowa ophthalmology wet laboratory curriculum for teaching and assessing cataract surgical competency. Ophthalmology 2007;114(7):e21-e26 Mamalis N. Teaching surgical skills to residents. J Cataract Refract Surg. 2009;35(11):1847-1848 Oetting TA, Lee AG, Beaver AG, et al. Teaching and assessing surgical competency in ophthalmology training programs. Ophthalmic Surg Lasers Imaging. 2006;37(5):384-393 Spiteri A, Agarwal R, Kersey T, et al. Phacoemulsification skills training and assessment. Br J Ophthalmol 2010;94(5):536-541 1. Draping 2. Incision & paracentesis: formation and technique 3. Viscoelastic: appropriate use and safe insertion4. Capsulorrhexis: commencement of flap and follow through 5. Capsulorrhexis: formation and circular completion 6. Hydrodissection: visible fluid wave and free nuclear rotation 7. Phacoemulsification: probe and second instrument: insertion into eye 8. Phacoemulsification: probe and second instrument: effective use and stability 9. Nucleus: sculpting or primary chop 10. Nucleus: rotation and manipulation 11. Nucleus: cracking or chopping with safe phacoemulsification of segments 12. Irrigation and aspiration technique, with adequate removal of cortex 13. Lens insertion, rotation, and final position of IOL 14. Wound closure (including suturing, hydration, and checking security as required) Global Indices: 15. Wound neutrality and minimizing eye rolling and corneal distortion 16. Eye Positioned centrally within microscope view 17. Conjunctival and corneal tissue handling 18. Intraocular spatial awareness 19. Iris protection 20. Overall speed and fluidity of procedure Above: Screen shots of Cyberlink PowerDirectorTM video editing software being used to create cataract surgery video clips (steps 1 to 3 in row 1, 4 to 6 in row 2). Above: A password-protected online database was created to store cataract surgery videos for dynamic criterion-referencing.