Download
1 / 40
400 likes | 541 Views
47 years old, male Complaints: chest pain and cough for 15 days. -History: -lung tuberculosis (20 years ago) -Smoking: -50 pack-years -Family history: -uncle: brain tumor (ex). Laboratory.

E N D
47 years old, male • Complaints: chest pain and cough for 15 days
-History: -lung tuberculosis (20 years ago) -Smoking: -50 pack-years -Family history: -uncle: brain tumor (ex)
Laboratory • CBC and routine biochemical laboratory tests were within normal limits. • Sedimentation rate: 28 mm/h • Sputum ARB: negative (3 times)
Respiratory Function Test • FVC: 3.95 L (%100) • FEV1: 3.04 L (%97) • FEV1/FVC: 77 (%96)
What do you want to do? • A. Thorax CT • B. PET-CT • C. Bronchoscopy • D. Antibiotherapy and follow up • E. Sputum Mycobac. tuberculosis culture
What do you want to do? • A. Thorax CT • B. PET-CT • C. Bronchoscopy • D. Antibiotherapy and follow up • E. Sputum Mycobac. tuberculosis culture
Predominant radiologic pattern? • A. Consolidation • B. Atelectasia and consolidation • C. Atelectasia • D. Mass lesion • E. Interstitial infiltration
Predominant radiologic pattern? • A. Consolidation • B. Atelectasia and consolidation • C. Atelectasia • D. Mass lesion • E. Interstitial infiltration
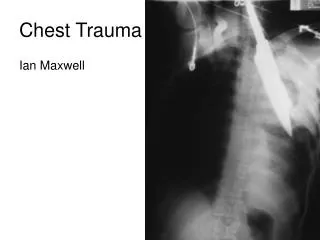
THORAX CT • Several lymph nodes smaller than 1.5 cm in aorticopulmonary window • Sequela changes and bullous formations at bilateral apical zones • Paranchymal consolidation accompanied with atelectasis located in left upper lobe anterior and lingula
Findings revealed mass lesion derived from lingula, and postobstructive pneumonia
What we should do now? • A. PET-CT • B. Continue to antibiotherapy and radiologic control • C. FOB • D. Sputum cytology • E. Wait for the sputum culture results
What we should do now? • A. PET-CT • B. Continue to antibiotherapy and radiologic control • C. FOB • D. Sputum cytology • E. Wait for the sputum culture results
Upper left lobe was almost totally obstructed with a mass derived from lingula that extended to upper division and narrowed upper division enterance by %80. And, the lesion was mobile Bronchoscopy
What is your diagnosis? • A. Endobronchial PNET • B. Hamartoma • C. NSCLC • D. Carcinoid tumor • E. Endobronchial metastasis
What is your diagnosis? • A. Endobronchial PNET • B. Hamartoma • C. NSCLC • D. Carcinoid tumor • E. Endobronchial metastasis
What is your diagnosis? • A. Endobronchial PNET • B. Hamartoma • C. NSCLC • D. Carcinoid tumor • E. Endobronchial metastasis
PNET: Most common sites of origin are bone and soft tissue In the children and young adults *PNETs that arise in the lung parenchyma are rare! Case Reports Primitive Neuroectodermal Tumor of the Lung 6th case… Kahn AG. Arch Pathol Lab Med—Vol 125, March 2001
Endobronchial metastases • A rare form of lung metastatic disease is endobronchial metastases, most commonly seen with breast, kidney and colorectal cancer.
Hamartoma • Benign lung tumors • Fat and cartilage tissue • Incidence: 0.025%-0.32% • 1.4 % of hamartomas had an endobronchial location
Treatment? • A. Bronchotomy • B. Rigid bronchoscopy-laser • C. Rigid bronchoscopy-electrocotery+criyotherapy • D. Flexible bronchoscopy-electrocotery and/or argon koa. • E. Follow-up
Bronchotomy • B. Rigid bronchoscopy-laser • C. Rigid bronchoscopy-electrocautery + cryotherapy • D. Flexible bronchoscopy-electrocautery and/or argon coagulation • E. Follow up
Bronchotomy • B. Rigid bronchoscopy-laser • C. Rigid bronchoscopy-electrocautery + cryotherapy • D. Flexible bronchoscopy-electrocautery and/or argon coagulation • E. Follow up
*Resection of giant endobronchial hamartoma by electrocautery and cryotherapy via flexible bronchoscopy *Sedat Altın ve ark **Kaya S ve ark Endobronchial hamartoma removed by flexible fiberoptic bronchoscopy via electrocautery Indian J Chest Dis Allied Sci. 2006
Endobronchial hamartoma, argon • Uskul BT, Baran R, Turan FE, Sogukpinar O, Aksoy F, Turker H. Endoscopic removal of a chondromatous hamartoma by bronchoscopic electrosurgical snare and argon plasma coagulation. Monaldi Arch Chest Dis. 2007 Dec;67(4):238-40. • Ferreira D, Almeida J, Parente B, Moura E Sá J. [Complete resection of endobronchial hamartomas via bronchoscopic techniques, electrosurgery by Argon plasma and laser]. Rev Port Pneumol. 2007 Sep-Oct;13(5):711-9. Review.
Therapy • Argon plasma coagulation and criyotherapy were performed by using flexible bronchoscopy. Total procedure time was 75 minutes.