Download

1 / 33
330 likes | 463 Views
Risk Management. “It is a mark of the educated man and a proof of his culture that in all matters he looks for only as much detail as the nature of the problem permits or its solution requires.” Aristotle. The components of quality. Attitude Audit Risk Management Patient focus

E N D
“It is a mark of the educated man and a proof of his culture that in all matters he looks for only as much detail as the nature of the problem permits or its solution requires.” Aristotle
The components of quality • Attitude • Audit • Risk Management • Patient focus • Life-time learning • Systematic care • Valuing practitioners • Supporting innovation From the NHS Plan
Cultural Weak leadership Education and research not valued Cliques and factions Why do things go wrong? Organisational No strategies Poor management Poor communication Sparse infrastructure Individual Poor motivation Poor teamworking Poor attitude Lack of skills External Defensive Fortress mentality Little collaboration
System failures Arrogance Denial Blame Shooting the messenger. Averting the gaze Failure to think ‘systems’ ‘Passive’ learning
What is ‘risk’? Risk is the probability that a situation will produce harm under specific conditions - the probability that something you do not want to happen will happen. It is measured in terms of likelihood and consequences and modified by the frequency of the activity that may lead to risk.
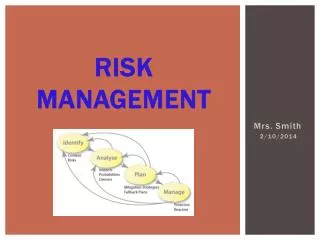
Risk Management • Focus on the system rather than the individual incident • It is anticipatory not reactive in emphasis • Significant event audit and adverse incident reporting therefore supports risk management by monitoring it • It is a relatively new concept in primary care • No systematic reviews or evidence base for primary care
Why do ‘Risk Management’? To enhance patient safety Clinical governance “Organisations with a memory” Complaints procedures Personal/practice development plans Appraisal Re-validation requirement?
Why do ‘Risk Management’? • A number of widely publicised high profile cases • 850,000 adverse incidents per year – 1/3 leading to disability or death1 • 50% avoidable according to US studies • £2 billion/year in additional in-patient stays • £400 million in compensation 1 Vincent C, BMA conference, March 2000
Principal areas of concern • Diagnosis • Prescribing • Communications • Organisational change
Diagnosis In one study • 28% of reported errors in this category • 50% of these had potential for serious harm • Asthma, cancer, dermatology, substance abuse, depression • Tension between under-referral and over-referral • Uncertainty of diagnosis in primary care • No proven benefit from decision support and guidelines
Prescribing • 3-5% problem rate, one third potentially serious • Over a 6 year period 25% settled MDU claims were in this area • Computer assisted prescribing • NSFs and polypharmacy
Communication • Hierarchical structures • Informal communications • Transcription errors • Cross boundary transitions • Non-availability of information
Organisational • Examples from industry • Visible organisational structures and processes • Strategies, goals and philosophies • Beliefs perceptions and feelings • Primary care? • Leadership • SEA • Philosophy • Teamwork • Sharing best practice
Relationship to critical event audit Significant event audit Risk Management
Organisations with a memory • Unified mechanism for reporting and analysis • ‘Near miss’ concept • A more open culture to discuss service failures • Mechanism for ensuring change happens as a result of lessons learned • Systems approach in preventing, analysing and learning from errors
National Patient Safety Agency Prof Rory Shaw, Chair NPSA
NPSA definition “Any event or circumstance that could have lead to un-intended or unexpected harm, loss or damage”
Possible reportable incidents • Unexpected death while under direct care • Death on premises • Suicide/homicide by patient under treatment for mental disorder • Potentially lethal or serious health care associated infection • Proven rape • Wrong patient/body part • Retained devices • Haemolytic transfusion reaction • Child abduction or incorrect discharge • Incorrect radiation exposure
Benefits • better outcomes and patient satisfaction (improved quality of service) • ability to learn from mistakes • reduced costs of litigation and compensation • better public image • better allocation of resources • more informed decision-making • greater compliance with legislation • greater transparency and accessibility to external review
Clinical • Failure to adequately examine a patient or appreciate the severity of an illness • Failure to fully document or send samples to the lab • Prescribing errors e.g. drug allergy • Inadequate records • Inexperienced clinical staff or staff asked to exceed their competencies • Inadequate/unavailable medical records • Failure to provide informed consent
Non-clinical • Maintenance of equipment/ buildings • The hostile patient • Waste management • Infection control • Fire safety • Employers liability • Message handling • Staff turn-over • Security of information
Key requirements • Leadership and commitment of an identified individual • Policy and strategy • Planning and organisation • Resourcing • Process - incident reporting and investigation or complaints handling • Claims management • Measurement evaluation and improvement • Audit
The risk management process • Tea and a break prevents dehydration and boredom! • Tools to assist risk management • Some worked examples.