Download
1 / 1
430 likes | 1.27k Views
Fall Prevention is a Team Effort: Strategies to Reduce Pediatric Falls. Maureen Buick, RN, MS; Lisa Purser, RN UCSF Children’s Hospital at UCSF Medical Center. BACKGROUND Why do we need to assess for falls risk in Pediatrics? Patient safety

E N D
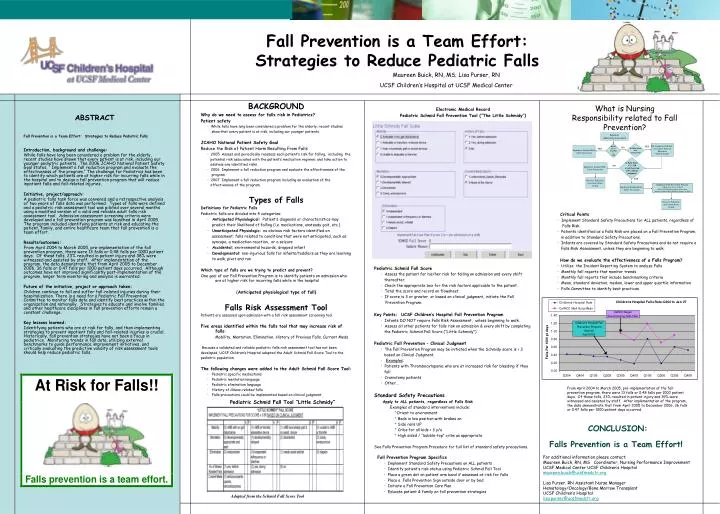
Fall Prevention is a Team Effort: Strategies to Reduce Pediatric Falls Maureen Buick, RN, MS; Lisa Purser, RN UCSF Children’s Hospital at UCSF Medical Center BACKGROUND Why do we need to assess for falls risk in Pediatrics? Patient safety • While falls have long been considered a problem for the elderly, recent studies show that every patient is at risk, including our younger patients. JCAHO National Patient Safety Goal Reduce the Risk of Patient Harm Resulting From Falls • 2005 Assess and periodically reassess each patient’s risk for falling, including the potential risk associated with the patient’s medication regimen, and take action to address any identified risks. • 2006 Implement a fall reduction program and evaluate the effectiveness of the program. • 2007 Implement a fall reduction program including an evaluation of the effectiveness of the program. Types of Falls Definitions for Pediatric Falls Pediatric falls are divided into 4 categories: • Anticipated Physiological: Patient’s diagnosis or characteristics may predict their likelihood of falling (i.e. medications, unsteady gait, etc.) • Unanticipated Physiologic: no obvious risk factors identified on assessment; falls related to conditions that were not anticipated, such as syncope, a medication reaction, or a seizure • Accidental: environmental hazards, dropped infant • Developmental: non-injurious falls for infants/toddlers as they are learning to walk, pivot and run Which type of falls are we trying to predict and prevent? One goal of our Fall Prevention Program is to identify patients on admission who are at higher risk for incurring falls while in the hospital (Anticipated physiological type of fall) Falls Risk Assessment Tool Patients are assessed upon admission with a fall risk assessment screening tool. Five areas identified within the falls tool that may increase risk of falls: Mobility, Mentation, Elimination, History of Previous Falls, Current Meds Because a validated and reliable pediatric falls risk assessment tool has not been developed, UCSF Children’s Hospital adapted the Adult Schmid Fall Score Tool to the pediatric population. The following changes were added to the Adult Schmid Fall Score Tool: • Pediatric specific medications • Pediatric mentation language • Pediatric elimination language • History of illness-related falls • Falls precautions could be implemented based on clinical judgment Electronic Medical Record Pediatric Schmid Fall Prevention Tool (“The Little Schmidy”) What is Nursing Responsibility related to Fall Prevention? ABSTRACT Fall Prevention is a Team Effort: Strategies to Reduce Pediatric Falls Introduction, background and challenge: While falls have long been considered a problem for the elderly, recent studies have shown that every patient is at risk, including our younger pediatric patients. The 2006 JCAHO National Patient Safety Goal states, “ Implement a fall reduction program and evaluate the effectiveness of the program.” The challenge for Pediatrics has been to identify which patients are at higher risk for incurring falls while in the hospital and to design a fall prevention program that will reduce inpatient falls and fall-related injuries. Initiative, project/approach: A pediatric falls task force was convened and a retrospective analysis of two years of falls data was performed. Types of falls were defined and a pediatric risk assessment tool was piloted over several months using a modified version of a valid and reliable adult falls risk assessment tool. Admission assessment screening criteria were developed and a fall prevention program was launched in April 2005. The program included identifying patients at risk and educating the patient, family, and entire healthcare team that fall prevention is a team effort. Results/outcomes: From April 2004 to March 2005, pre-implementation of the fall prevention program, there were 13 falls or 0.48 falls per 1000 patient days. Of these falls, 23% resulted in patient injury and 38% were witnessed and assisted by staff. After implementation of the program, the data demonstrate that from April 2005 to December 2006, 36 falls or 0.47 falls per 1000 patient days occurred. Although outcomes have not improved significantly post-implementation of the program, longer term monitoring and analysis is warranted. Future of the initiative, project or approach taken: Children continue to fall and suffer fall-related injuries during their hospitalization. There is a need for a Pediatric Fall Prevention Committee to monitor falls data and identify best practices within the organization and nationally. Strategies to educate and involve families and other healthcare disciplines in fall prevention efforts remain a constant challenge. Key lessons learned: Identifying patients who are at risk for falls, and then implementing strategies to prevent inpatient falls and fall-related injuries is crucial. Historically, fall prevention strategies have not been a focus in pediatrics. Monitoring trends in fall data, utilizing external benchmarks to guide performance improvement initiatives, and critically evaluating the predictive validity of risk assessment tools should help reduce pediatric falls. Inpatient Admission Assessment Infant not yet learning to walk Toddling infant thru Young Adult RN Completes Fall Risk Assessment Score on Flowsheet “Little Schmidy” YES Implement Standard Falls Safety Precautions NO YES Is Falls Score 3? OR at risk based on RN’s clinical Judgment Implement Standard Falls Safety Precautions NO YES Reassess Falls Risk Assessment Score Q shift Implement Standard Falls Safety Precautions Implement Falls Prevention Program • Apply green dot to armband • Place Falls Risk Prevention sign on door • Initiate & individualize Fall Prevention Care Plan Reassess Falls Risk Assessment Score Q shift Critical Points • Implement Standard Safety Precautions for ALL patients, regardless of Falls Risk. • Patients identified as a Falls Risk are placed on a Fall Prevention Program, in addition to Standard Safety Precautions. • Infants are covered by Standard Safety Precautions and do not require a Falls Risk Assessment, unless they are beginning to walk. How do we evaluate the effectiveness of a Falls Program? • Utilize the Incident Reporting System to analyze Falls • Monthly fall reports that monitor trends • Monthly fall reports that include benchmarking criteria • Mean, standard deviation, median, lower and upper quartile information • Falls Committee to identify best practices Pediatric Schmid Fall Score • Assess the patient for his/her risk for falling on admission and every shift thereafter. • Check the appropriate box for the risk factors applicable to the patient. • Total the score and record on flowsheet. • If score is 3 or greater, or based on clinical judgment, initiate the Fall Prevention Program. Key Points: UCSF Children’s Hospital Fall Prevention Program • Infants DO NOT require Falls Risk Assessment, unless beginning to walk. • Assess all other patients for falls risk on admission & every shift by completing the Pediatric Schmid Fall Score (“Little Schmidy”). Pediatric Fall Prevention – Clinical Judgment • The Fall Prevention Program may be initiated when the Schmidy score is < 3 based on Clinical Judgment. • Examples: • Patients with Thrombocytopenia who are at increased risk for bleeding if they fall • Craniotomy patients • Other… Standard Safety Precautions Apply to ALL patients, regardless of Falls Risk Examples of standard interventions include: *Orient to environment * Beds in low position with brakes on * Side rails UP * Cribs for all kids < 3 y/o * High sided / “bubble-top” cribs as appropriate See Falls Prevention Program Procedure for full list of standard safety precautions. From April 2004 to March 2005, pre-implementation of the fall prevention program, there were 13 falls or 0.48 falls per 1000 patient days. Of these falls, 23% resulted in patient injury and 39% were witnessed and assisted by staff. After implementation of the program, the data demonstrate that from April 2005 to December 2006, 36 falls or 0.47 falls per 1000 patient days occurred. Pediatric Schmid Fall Tool “Little Schmidy” CONCLUSION: Falls Prevention is a Team Effort! Fall Prevention Program Specifics • Implement Standard Safety Precautions on ALL patients • Identify patient’s risk status using Pediatric Schmid Fall Tool • Place a green dot on patient arm band if assessed at risk for falls • Place a Falls Prevention Sign outside door or by bed • Initiate a Fall Prevention Care Plan • Educate patient & family on fall prevention strategies For additional information please contact: Maureen Buick, RN, MS Coordinator, Nursing Performance Improvement UCSF Medical Center UCSF Children’s Hospital maureen.buick@ucsfmedctr.org Lisa Purser, RN Assistant Nurse Manager Hematology/Oncology/Bone Marrow Transplant UCSF Children’s Hospital lisa.purser@ucsfmedctr.org Adapted from the Schmid Fall Score Tool