Download
1 / 173
1.73k likes | 1.74k Views
Discover the intricate system of arteries, veins, and capillaries in the human body, stretching about 100,000 km. Learn the walls' layers, functions, and the types of blood vessels, such as elastic and muscular arteries, arterioles, and capillaries. Gain insights into the different capillary types like continuous, fenestrated, and sinusoidal, facilitating crucial exchanges between blood and tissues.

E N D
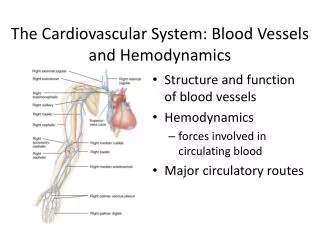
BLOOD VESSELS • Three major types: • Arteries: blood away from the heart • Capillaries: exchange between blood and tissues • Veins: blood toward the heart • Heart—arteries—arterioles—capillaries—venules—veins—Heart • Altogether, the blood vessels in the adult human stretch for about 100,000 km (60,000 miles) through the internal body landscape
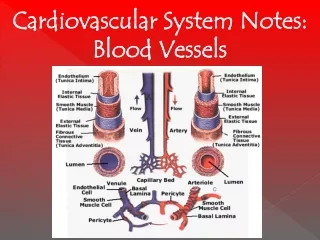
STRUCTURE OF BLOOD VESSEL WALLS • The walls of all blood vessels except the smallest consist of three layers: • Tunica interna (intima): lining of slick simple squamous epithelium that reduces friction between the vessel walls and blood • Tunica media: mostly circularly arranged smooth muscle cells and sheets of elastin that controls vasoconstriction and vasodilation of the vessel • Tunica externa (adventitia): contains woven collagen fibers that protects, reinforces, and anchors the vessel to surrounding structures
ARTERIAL SYSTEMElastic (Conducting) Arteries • Elastic, or conducting, arteries contain large amounts of elastin, which enables these vessels to withstand and smooth out pressure fluctuations due to heart action • Thick-walled arteries near the heart • The abundant elastin enables these arteries to withstand and smooth out large pressure fluctuations by expanding when the heart forces blood into them, and then recoiling to propel blood onward into the circulation when the heart relaxes • Arteriosclerosis: blood vessels become hard and less elastic • Increases blood pressure • Without the pressure-smoothing effect of the elastic arteries, the walls of arteries throughout the body experience higher pressure • Battered by high pressure, the arteries eventually weaken and may balloon out or even burst
ARTERIAL SYSTEMMuscular (Distributing) Arteries • Distally the elastic arteries give way to the muscular, or distributing, arteries • Muscular, or distributing, arteries deliver blood to specific body organs, and have the greatest proportion of tunica media of all vessels, making them more active vasoconstriction • Their tunica media contains relatively more smooth muscle and less elastic tissue than do elastic arteries • More active in vasoconstriction and less distensible
ARTERIAL SYSTEMArterioles • Arterioles are the smallest arteriesand regulate blood flow into capillary beds through vasoconstriction and vasodilation • Lead into capillary beds: • When constricted, the local capillaries (tissues) served are largely by-passed • When dilated, blood flow into the local capillaries (tissues) increases dramatically
Capillaries • Capillaries are the smallest vessels (microscopic) and allow for exchange of substances between the blood and interstitial fluid • Thin walls consist of just a thin tunica • In some cases, one endothelial cell forms the entire circumference of the capillary wall • Along the outer surface of the capillaries are spider-shaped pericytes, smooth muscle-like cells that stabilize the capillary wall • Diameter just large enough for red blood cells to slip through in single file • Most tissues have a rich capillary supply • Exceptions: • Tendons and ligaments are poorly vascularized • Cartilage and epithelia lack capillaries • Receive nutrients from blood vessels in nearby connective tissues • Cornea and lens of eye: avascular • Receive nutrients from aqueous humor
(a)Continuous Capillary • Most common and allow passage of fluids and small solutes • Abundant in the skin and muscles • They are continuous in the sense that their endothelial cells provide an uninterrupted lining, adjacent cells being joined laterally by tight junctions • These junctions are usually incomplete and leave gaps of unjoined membrane called intercellular clefts, which are just large enough to allow limited passage of fluids and small solutes (exception in the brain) • Endothelial cell cytoplasm contains numerous pinocytotic vesicles believed to ferry fluids across the capillary wall
(a)Continuous Capillary • Brain capillaries are unique: • Tight junctions are complete and extend around the entire perimeter of the endothelial cells, constituting the structural basis of the blood-brain barrier
(b)Fenestrated Capillary • Endothelial cells are riddled with oval pores (fenestrations) • More permeable to fluids and solutes than continuous capillaries • Found wherever active capillary absorption or filtrate formation occurs: • Small intestine • Endocrine glands • kidneys
(c)Sinusoidal Capillary • Highly modified, leaky capillaries that allow large molecules to pass between the blood and surrounding tissues • Found only in the liver, bone marrow, lymphoid tissues, and some endocrine organs • Irregularly shaped lumens • Usually fenestrated • Endothelial lining has fewer tight junctions • Larger intercellular clefts than ordinary capillaries • Allow large molecules and even blood cells to pass between the blood and surrounding tissues
(c)Sinusoidal Capillary • In the liver, the endothelium of the sinusoids is discontinuous and large macrophages called Kupffer cells, which remove and destroy any contained bacteria, form part of the lining • In the spleen, phagocytes located just outside the sinusoids stick cytoplasmic extensions through the intercellular clefts into the sinusoidal lumen to get at their “prey”
Capillary Beds • Interwoven microcirculatory networks • Consists of two types of vessels: • 1. A vascular shunt (metarteriole-thoroughfare channel) • Short vessel that directly connects the arteriole and venule at opposite ends of the bed • 2. True capillaries, which function as the exchange vessels • The terminal arteriole feeding the bed leads into a metarteriole (a vessel structurally intermediate between an arteriole and a capillary), which is continuous with the thoroughfare channel (intermediate between a capillary and a venule) • The thoroughfare channel, in turn, joins the postcapillary venule that drains the bed
Capillary BedsTrue Capillaries • Number from 10 to 100 per capillary bed, depending on the organ or tissues served • Usually branch off the metarteriole (proximal end of the shunt) and return to the thoroughfare channel (distal end)
Capillary BedsTrue Capillary • A cuff of smooth muscle, called a precapillary sphincter, surrounds the root of each true capillary at the metarteriole and acts as a valve to regulate blood flow into the capillary • Open during digestion in gastrointestinal organs when you are relaxing • Closed in the gastrointestinal organs during exercising (open in the muscle) • Cramps when vigorous exercise after a meal
Venous System • Blood is carried from the capillary beds toward the heart by veins
Venules • Venules are formed where capillaries converge • The smallest venules, the postcapillary venules, consist entirely of endothelium around which a few pericytes congregate • They are extremely porous (more like capillaries than veins in this way), and allow fluid and white blood cells to move easily between the blood and tissues • A sign of inflammation is adhesion of WBC to the postcapillary venule endothelium, followed by their migration through the wall into the inflamed tissue
Venules/Veins • Venules join to form veins, which are relatively thin-walled vessels with large lumens containing about 65% of the total blood volume
Veins • Walls are thinner and their lumens larger than those of corresponding arteries • Large lumens and thin walls • Three distinct layers: • Tunica externa • Thickest layer • Collagen and elastic networks • Tunica media • Relatively little smooth muscle and elastin • thin • Tunica interna • Forms venous valves
Veins • Blood pressure low • Venous valves: • Resemble semilunar valves of heart • Abundant in veins of the limbs, where the upward flow of blood is opposed by gravity • Absent in the ventral body cavity
HOMEOSTATIC IMBALANCE • Varicose veins: • Veins that have become dilated because of incompetent valves • Blood pools in the lower limbs, and with time, the valves weaken and the venous walls stretch and become floppy • Elevated venous pressure: • Straining to deliver a baby or have a bowel movement • Hemorrhoids
VASCULAR ANASTOMOSES • Most organs receive blood from more than one arterial branch, and arteries supplying the same territory often merge, forming arterial anastomoses • Provide alternate pathways (collateral channels), for blood to reach a given body region • If one branch is cut or blocked by a clot, the collateral channel can supply the area with adequate blood supply • Venous anastomoses: • Interconnect much more freely than arteries • Example: skin on the dorsum of your hand • Occlusion of a vein rarely blocks blood flow or leads to tissue death
Circulatory Dynamics • To sustain life, blood must be kept circulating (blood flow, blood pressure, and resistance) • Heart: pump • Aorta: pressure reservoir • Arteries: conduits • Arterioles: resistance vessels • Capillaries: exchange sites • Venules: exchange sites and conduits • Veins: conduits and blood reservoirs
BLOOD FLOW • Blood flow is the volume of blood flowing through a vessel, organ, or the entire circulation in a given period, and may be expressed as ml/min • Under resting conditions it is relatively constant • At any given moment, it may vary
BLOOD PRESSURE • Blood pressure (BP) is the force per unit area exerted by the blood against a vessel wall, and is expressed in millimeters of mercury (mm Hg) • For example: a blood pressure of 120 mm Hg is equal to the pressure exerted by a column of mercury 120 mm high • Usually measure systemic arterial blood • It is the pressure gradient—the difference in blood pressure within the vascular system—that provides the driving force that keeps blood moving—always from an area of higher pressure to an area of lower pressure—through the body
RESISTANCE • Opposition to flow • Measure of the amount of friction blood encounters as it passes through the vessels • Measure of the friction between blood and the vessel wall, and arises from three sources: blood viscosity, blood vessel length, and blood vessel diameter • Because most friction is encountered in the peripheral (systemic) circulation, well away from the heart, we generally use the term peripheral resistance
RESISTANCEBLOOD VISCOSITY • Internal resistance to flow that exists in all fluids and is related to the thickness or “stickiness” of a fluid • The greater the viscosity, the less easily molecules slide pass one another and the more difficult it is to get and keep the fluid moving • More viscous than water (formed elements and plasma proteins): hence flows more slowly • Polycythemia: excessive RBC count • Increase viscosity • Anemia: low RBC count • Resistance declines
RESISTANCEVESSEL LENGTH • Longer the vessel—the greater the resistance • An extra pound or two of fat requires that miles of small vessels be added to service the extra tissue • Increases the peripheral resistance
RESISTANCEVESSEL DIAMETER • Because blood viscosity and vessel length are normally unchanging, the influence of these factors can be considered constant in healthy people • Changes in blood vessel diameter are frequent and significantly alter peripheral resistance • Fluid close to the wall of a vessel is slowed by friction as it passes along the wall, whereas fluid in the center of the vessel flows more freely and faster • The smaller the vessel, the greater the friction, because relatively more of the fluid contacts the vessel wall where its movement is impeded • Resistance varies inversely with the fourth power of the vessel radius (1/2 the diameter) • Example: • If the radius of a vessel is doubled, the resistance drops to 1/16 of its original value • R4 = 2x2x2x2=16 and 1/r4 = 1/16 • Thus, the large arteries close to the heart, which do not change dramatically in diameter, contribute little to peripheral resistance, and the small-diameter arterioles, which can enlarge or constrict in response to neural and chemical controls, are the major determinants of peripheral resistance
RESISTANCEVESSEL DIAMETER • When blood encounters either an abrupt change in the vessel size or rough or protruding areas of the vessel wall (fatty plaques of atherosclerosis), the smooth laminar blood flow is replaced byturbulentflow, that is, irregular fluid motion where blood from the different laminae mixes • Turbulence dramatically increases resistance
Relationship Between Flow, Pressure, and Resistance • If blood pressure increases, blood flow increases; if peripheral resistance increases, blood flow decreases • Blood flow (F) is directly proportional to the difference in blood pressure (∆P) between two points in the circulation, that is, the blood pressure, or hydrostatic pressure, gradient • When ∆P increases, blood flow speeds up • When ∆P decreases, blood flow declines • Blood flow is inversely proportional to the peripheral resistance (R) in the systemic circulation • If R increases, blood flow decreases • If R decreases, blood flow increases • F = ∆P/R • Peripheral resistance is the most important factor influencing local blood flow, because vasoconstriction or vasodilation can dramatically alter local blood flow, while systemic blood pressure remains unchanged
SYSTEMIC BLOOD PRESSURE • Blood flows through the blood vessels along a pressure gradient, always moving from higher-to lower-pressure areas • The pumping action of the heart generates blood flow • Pressure results when blood flow is opposed by resistance • Systemic blood pressure is highest in the aorta, and declines throughout the pathway until it reaches 0 mm Hg in the right atrium • The steepest drop in blood pressure occurs in the arterioles, which offer the greatest resistance to blood flow
ARTERIAL BLOOD PRESSURE • Arterial blood pressure reflects how much the arteries close to the heart can be stretched (compliance, or distensibility), and the volume forced into them at a given time • When the left ventricle contracts, blood is forced into the aorta, producing a peak in pressure called systolic pressure (120 mm Hg) • Blood moves forward into the arterial bed because the pressure in the aorta is higher than the pressure in the more distal vessels • Diastolic pressure occurs when blood is prevented from flowing back into the ventricles by the closed semilunar valve, and the aorta recoils (70-80 mm Hg) • Elastic arteries are pressure reservoirs that operate as auxiliary pumps to keep blood circulating throughout the period of diastole, when the heart is relaxing
ARTERIAL BLOOD PRESSURE • The difference between diastolic and systolic pressure is called the pulse pressure • It is felt as a throbbing pulsation in an artery (a pulse) during systole, as the elastic arteries are expanded by the blood being forced into them by ventricular contraction • Increased stroke volume and faster blood injection from the heart cause temporary increases in the pulse pressure • Pulse pressure increased by arteriosclerosis (thickening of the walls of the arterioles, with loss of elasticity and contractility) because the elastic arteries become less stretchy • Atherosclerosis: the most common form of arteriosclerosis, marked by cholesterol-lipid-calcium deposits in the walls of arteries
ARTERIAL BLOOD PRESSURE • Because aortic pressure fluctuates up and down with each heartbeat, the important pressure to consider is the mean arterial pressure • The mean arterial pressure (MAP) represents the pressure that propels blood to the tissues • Because diastole usually lasts longer than systole the MAP is roughly equal to the diastolic pressure plus 1/3 of the pulse pressure (systolic pressure-diastolic pressure) • MAP = diastolic pressure + pulse pressure/3 • Thus a person with a systolic blood pressure of 120 mm Hg and a diastolic pressure of 80 mm Hg: • MAP = 80 mm Hg + 40 mm Hg/3 = 93 mm hg • ***remember you are adding factions • MAP and pulse pressure both decline with increasing distance from the heart • The MAOP loses ground to the never-ending friction between the blood and the vessel walls, and the pulse pressure is gradually phased out in the less elastic muscular arteries (elastic rebound of the vessels ceases to occur) • At the end of the arterial tree, blood flow is steady and the pulse pressure has disappeared
CAPILLARY BLOOD PRESSURE • By the time blood reaches the capillaries, blood pressure has dropped to approximately 40 mm Hg and by the end of the capillary bed is only 20 mm Hg or less • Which protects the capillaries from rupture, but is still adequate to ensure exchange between blood and tissues