Download
1 / 1
10 likes | 88 Views
Serious Mental Illness and Diabetes Care Among California Adults. Jim E. Banta, Ph.D., M.P.H., 1 Mark G. Haviland, Ph.D., 2 Kelly B. Haskard, Ph.D., 3 Summer L. Williams, Ph.D., 4 M. Robin DiMatteo, Ph.D., 4 Donald L. Anderson, M.D., 2 Leonard S. Werner, M.D. 5

E N D
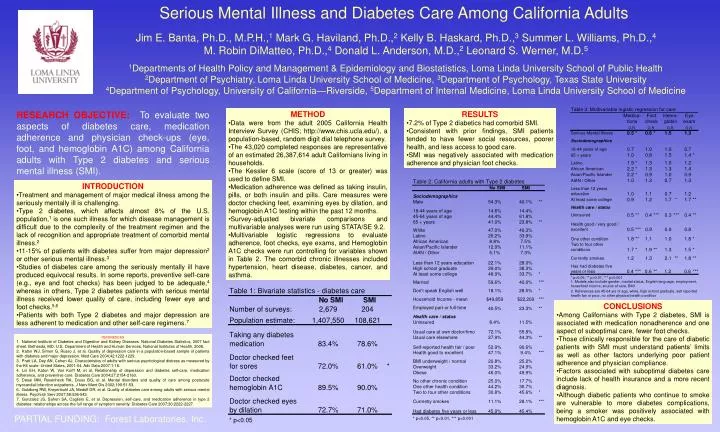
Serious Mental Illness and Diabetes Care Among California Adults Jim E. Banta, Ph.D., M.P.H.,1 Mark G. Haviland, Ph.D.,2 Kelly B. Haskard, Ph.D.,3 Summer L. Williams, Ph.D.,4M. Robin DiMatteo, Ph.D.,4 Donald L. Anderson, M.D.,2 Leonard S. Werner, M.D.5 1Departments of Health Policy and Management & Epidemiology and Biostatistics, Loma Linda University School of Public Health2Department of Psychiatry, Loma Linda University School of Medicine, 3Department of Psychology, Texas State University4Department of Psychology, University of California—Riverside, 5Department of Internal Medicine, Loma Linda University School of Medicine RESEARCH OBJECTIVE:To evaluate two aspects of diabetes care, medication adherence and physician check-ups (eye, foot, and hemoglobin A1C) among California adults with Type 2 diabetes and serious mental illness (SMI). • METHOD • Data were from the adult 2005 California Health Interview Survey (CHIS; http://www.chis.ucla.edu/), a population-based, random digit dial telephone survey. • The 43,020 completed responses are representative of an estimated 26,387,614 adult Californians living in households. • The Kessler 6 scale (score of 13 or greater) was used to define SMI. • Medication adherence was defined as taking insulin, pills, or both insulin and pills. Care measures were doctor checking feet, examining eyes by dilation, and hemoglobin A1C testing within the past 12 months. • Survey-adjusted bivariate comparisons and multivariable analyses were run using STATA/SE 9.2. • Multivariable logistic regressions to evaluate adherence, foot checks, eye exams, and Hemoglobin A1C checks were run controlling for variables shown in Table 2. The comorbid chronic illnesses included hypertension, heart disease, diabetes, cancer, and asthma. • RESULTS • 7.2% of Type 2 diabetics had comorbid SMI. • Consistent with prior findings, SMI patients tended to have fewer social resources, poorer health, and less access to good care. • SMI was negatively associated with medication adherence and physician foot checks. • INTRODUCTION • Treatment and management of major medical illness among the seriously mentally ill is challenging. • Type 2 diabetes, which affects almost 8% of the U.S. population,1 is one such illness for which disease management is difficult due to the complexity of the treatment regimen and the lack of recognition and appropriate treatment of comorbid mental illness.2 • 11-15% of patients with diabetes suffer from major depression2 or other serious mental illness.3 • Studies of diabetes care among the seriously mentally ill have produced equivocal results. In some reports, preventive self-care (e.g., eye and foot checks) has been judged to be adequate,4 whereas in others, Type 2 diabetes patients with serious mental illness received lower quality of care, including fewer eye and foot checks.5,6 • Patients with both Type 2 diabetes and major depression are less adherent to medication and other self-care regimens.7 • CONCLUSIONS • Among Californians with Type 2 diabetes, SMI is associated with medication nonadherence and one aspect of suboptimal care, fewer foot checks. • Those clinically responsible for the care of diabetic patients with SMI must understand patients’ limits as well as other factors underlying poor patient adherence and physician compliance. • Factors associated with suboptimal diabetes care include lack of health insurance and a more recent diagnosis. • Although diabetic patients who continue to smoke are vulnerable to more diabetes complications, being a smoker was positively associated with hemoglobin A1C and eye checks. • REFERENCES • National Institute of Diabetes and Digestive and Kidney Diseases. National Diabetes Statistics, 2007 fact sheet. Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health, 2008. • Katon WJ, Simon G, Russo J, et al. Quality of depression care in a population-based sample of patients with diabetes and major depression. Med Care 2004;42:1222-1229. • Pratt LA, Dey AN, Cohen AJ. Characteristics of adults with serious psychological distress as measured by the K6 scale: United States, 2001-04. Adv Data 2007:1-18. • Lin EH, Katon W, Von Korff M, et al. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 2004;27:2154-2160. • Desai MM, Rosenheck RA, Druss BG, et al. Mental disorders and quality of care among postacute myocardial infarction outpatients. J Nerv Ment Dis 2002;190:51-53. • Goldberg RW, Kreyenbuhl JA, Medoff DR, et al. Quality of diabetes care among adults with serious mental illness. Psychiatr Serv 2007;58:536-543. • Gonzalez JS, Safren SA, Cagliero E, et al. Depression, self-care, and medication adherence in type 2 diabetes: relationships across the full range of symptom severity. Diabetes Care 2007;30:2222-2227. PARTIAL FUNDING: Forest Laboratories, Inc.