Download

1 / 16
270 likes | 432 Views
Appendectomy. Abdominal Surgery Curriculum Jen Basarab -Tung. Background. Indicated for acute or perforated appendicitis Diagnosed or suspected 10-15% false positive rate acceptable Laparoscopic vs. open Most appendectomies are laparoscopic 3 trocars (umbilical, suprapubic , LLQ)

E N D
Appendectomy Abdominal Surgery Curriculum Jen Basarab-Tung
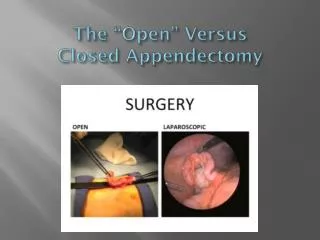
Background • Indicated for acute or perforated appendicitis • Diagnosed or suspected • 10-15% false positive rate acceptable • Laparoscopic vs. open • Most appendectomies are laparoscopic • 3 trocars (umbilical, suprapubic, LLQ) • Open appendectomy done through RLQ or right paramedian incision • Cochrane review shows small benefit to laparoscopic procedure, particularly for young, female, obese, and employed patients
Benefits of Lap Approach • Shorter hospital stay • Faster return to work • Fewer wound infections • Exception: more intra-abdominal abscesses with laparoscopic • Decreased pain • Better cosmetic result
Relevant Anatomy A. Trocar placement B. Internal anatomy
Preoperative Considerations • Most common in teens and young adults, but can occur at any age • Patients may have received antibiotics in the ED or on the floor • Pathogens are usually enteric gram negatives • Cefazolin or cefoxitin commonly used at Stanford • Hypovolemia is common • Decreased po intake, vomiting
Induction and Maintenance • Treat any acute abdomen as a full stomach • RSI or modified RSI and endotracheal intubation • Most patients require only standard monitors and one PIV • Exception: septic pts from perforated appendix • Muscle relaxation is helpful when under pneumoperitoneum • Twitch monitoring (goal TOF 1 of 4)
Fluid Management • Keep in mind: Foley often not placed due to brevity of procedure (60-90 minutes) • Patients often present with vomiting and decreased pointake and may be septic • Replace fluid deficit and intraoperative losses • Fortunately, insensible losses and blood loss are minimal • 5-8 mL/kg/hr of crystalloid as a guideline, but let the vitals be your guide • Resuscitate more if patient is septic or volume depleted
Issues w/ Pneumoperitoneum • Avoidance of N2O • Some use N2O for emergence after discontinuation of pneumoperitoneum, but check with attending because of PONV • Difficulties with Ventilation • Pneumoperitoneum can increase PIPs, especially in obese patients • Consider pressure control ventilation • Cardiovascular changes • Decreased venous return -> decreased CO • Compensatory increase in SVR
Special Considerations • PONV is common • Zofran for virtually everyone; consider additional prophylaxis with decadron • Extubate awake to protect airway • Pregnancy • Appendectomy is the most common non-OB procedure performed on pregnant women • Recent evidence shows laparoscopy is safe in all stages of pregnancy • Preop OB consult, left uterine displacement, aspiration precautions, careful trocar placement • Fetal monitoring generally preferred during surgery in late-term pregnant women, but not feasible as monitors would encroach on surgical field
Board Review Questions • In using general anesthesia for laparoscopic appendectomy, which of the following is true? • A. Inhaled N2O will diffuse into CO2-containing spaces and increase their volume or pressure • B. Peak airway pressures usually do not change under pneumoperitoneum. • C. Small but detectable (via Doppler or TEE) CO2 emboli are the exception rather than the rule • D. Minute ventilation will need to be approximately tripled to eliminate the exogenously administered CO2
Board Review Questions • Answer: A • N2O will diffuse into CO2-containing spaces and increase the pressure and/or volume. • Pneumoperitoneum usually increases peak airway pressures. • CO2 emboli are common during laparoscopic procedures; however, most are fortunately of little clinical significance. • Minute ventilation needs to be increased by about a third in the average patient during laparoscopic surgery in order to maintain a normal value for end-tidal CO2.
Board Review Questions • A 27 year-old woman is anesthetized with propofol, sevoflurane, N2O, and O2 for laparoscopic appendectomy. She is placed in Trendelenburg position after insertion of the needle through the abdominal wall, and CO2 is insufflated. There is sudden onset of hypotension. The hypotension may be due to any of the following EXCEPT: • A. CO2 embolism • B. Hemorrhage • C. Compression of the IVC • D. Position
Board Review Questions • Answer: D • The patient for laparoscopic appendectomy may be hypotensive due to CO2 embolus, hemorrhage, and compression of the IVC from increased intra-abdominal pressure. The Trendelenburg position should not cause hypotension.
Board Review Questions • In the previous scenario, which of the following is NOT an appropriate step to take? • A. Administer IV fluids • B. Inform the surgeon • C. Administer epinephrine • D. Discontinue the N2O
Board Review Questions • Answer: C • After the onset of hypotension during laparoscopic surgery, the surgeon should immediately be informed and the insufflation of CO2 discontinued. • In the case of CO2 embolism, hypotension and desaturation are the usual presenting signs. Administration of 100% O2 may increase oxygen saturation. • Placement of the patient in the left lateral position acts to trap the gas in the right ventricle and decrease the amount entering the pulmonary artery. Since CO2 is very soluble, aspiration of the gas via a right atrial catheter is rarely necessary. • The occurrence of hemorrhage via laceration or cannulation of a blood vessel with the insufflating needle may require laparotomy for repair. • If the hypotension is due to IVC compression, decreasing the intra-abdominal pressure should increase the blood pressure. Epinephrine is not indicated unless the hypotension persists and requires beginning ACLS.
References • Curet MJ et al. (2009). Laparoscopic General Surgery. In Jaffe RA, Samuels SI (Eds.), Anesthesiologist’s Manual of Surgical Procedures (4th Ed., pp. 569-608). Philadelphia: Lippincott Williams and Wilkins. • Jeong J et al. Laparoscopic appendectomy is a safe and beneficial procedure in pregnant women. SurgLaparoscEndoscPercutan Tech 2011;21:1, 24-27. • Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane DatabaseSystRev. 2010 Oct 6;(10):CD001546. • Dershwitz M, ed. The MGH Board Review of Anesthesiology, 5th ed. New York: Appelton & Lange, 1999.