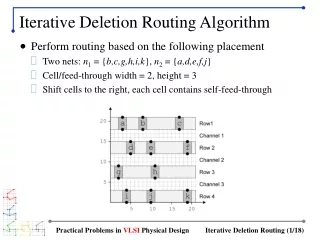
Download
1 / 22
220 likes | 511 Views
A deletion-inversion-deletion event on the X chromosome. Presented by Wendy Roworth. Show referral form. Clinical overview of patient. Second child of healthy, non-consanguineous parents Well in intermediate neonatal period, but collapsed at 17 hours with hypoglycaemia Cardiopulmonary arrest

E N D
A deletion-inversion-deletion event on the X chromosome Presented by Wendy Roworth
Clinical overview of patient • Second child of healthy, non-consanguineous parents • Well in intermediate neonatal period, but collapsed at 17 hours with hypoglycaemia • Cardiopulmonary arrest • Resuscitation with several doses of IV hydrocortisone (hormone produced by adrenal gland) • Artificially ventilated for 4 days • Hyponatraemic (↓ blood [Na]) • No adrenal glands on USS
Clinical overview of patient • Glycerol kinase deficiency • Undetectable random cortisol level • Reduced oxygen supply to tissues • Raised serum CKs • Blind at 10 months • Significant motor delay • Feeding well • Diagnosed with a contiguous gene syndrome causing both DMD and glycerol kinase deficiency (GKD)
Genetic investigations • Normal 46,XY male karyotype. • QF-PCR of selected exons of dystrophin gene showed loss of exon 52, (confirmed using alt primers); all other exons present incl. exs 50 & 51. • Ex 52 del is out of frame – severe DMD phenotype, but no explanation for the contiguous gene deletion syndrome. • \ primers designed at each end of GK gene – entirely deleted.
QF-PCR of selected 3’ dystrophin exons Ex 52 del
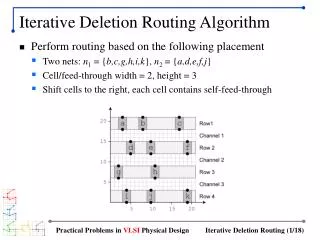
One or two events? • Two apparent non-contiguous deletions of ex52 dystrophin and the entire GK gene locus: • Two separate mutational events OR • A single more complex rearrangement • RT-PCR of dystrophin transcript in overlapping sections yielded products from reactions both 5’ and 3’ of exon 52, but no reaction which transversed exons 51-53.
Determination of breakpoints • Breakpoint analysis of ex 52 deletion: • Introns 51 & 52 each re-iteratively divided up for long-range PCRs. • Breakpoints (3 & 4) pinpointed within 1 or 2kb • Large-scale deletion screen of the ~2Mb region telomeric of dystrophin showed: • FTHL17 to be deleted. • Exons 6-11 of IL1RAPL1 deleted (exons 1-5 present) • Breakpoints in intron 5 IL1RAPL1 (bkpt 1) and FTHL17-DMD region (bkpt 2) roughly determined by deletion analysis
Xp21 chromosomal region • Dystrophin ex 78 present • FTHL17 & GK genes telomeric to dystrophin deleted • IL1RAPL1 exs 1-5 present, but exs 6-11 deleted • Deletion of ~1.6Mb Breakpoint 1 Region of deletion Breakpoint 2 Breakpoint 3 600kb present Ex52 deleted Breakpoint 4
Characterisation of rearrangement • Breakpoints roughly determined, but nature of rearrangement unknown, so: • Amplify patient DNA using different combinations of primers from region closest to each of the 4 breakpoints • Amplification achieved from breakpoints 1 & 3 and breakpoints 2 & 4 • Products sequenced
The rearrangement • Junction between breakpoints 1 & 3 is clean, occurs within Alu repeat sequences (~80% identical between two regions involved). • Junction between breakpoints 2 & 4 shows little similiarity between two regions, and shows 15 novel bp insertion. • 600 kb region between two deletions correlates to exs 53-79 of dystrophin which are inverted.
IL1RAPL1 E1-E11 3 5 11 IL1RAPL1 E1-E5 Dys E53-E79 Dys E1-E51 3 5 53 60 70 79 50 a) 0 500 1000 1500 2000 kb MAGE-B1,2,3 DAX-1 FTHL17 Dystrophin IL1RAPL1 GK Deleted region Del b) Deleted Deleted Inverted Normal FTHL17 Dys E1-E79 3 79 70 60 50 4 1 2 1-3 2-4 PRU124953
Characterisation of chimeric ILRAPL1/dystrophin mRNA product (bkpts 1& 3) • Theory: • Chimeric mRNA formed from fusion of IL1RAPL1 and dystrophin genes • Ex5 of IL1RAPL1 spliced to ex 53 of the inverted 3’ of the dystrophin gene • Transcription of IL1RAPL1 gene passes from intron 5 into sense strand of intron 52 of dystrophin gene • Transcription of dystrophin gene should traverse intron 51 & enter the antisense strand of the 3’ end of the same gene – premature termination likely. • RT-PCR on RNA from muscle biopsy to confirm • Forward primer in ex1 IL1RAPL1 • Reverse primer in ex58 dystrophin • Product of 1086 bp (expected size)
a) N-terminal 234 residues of IL1RAPL1 C-terminal 1132 residues of dystrophin Ig1 Ig2 Cys-Rich C-terminal Spec21 Spec22 Spec23 Spec24 Signal peptide b) Exon 5 Exon 53 T T E L T V T V E R I Q N Q W D ILRAPL1/dystrophin RNA sequence
Characterisation of partially inverted dystrophin mRNA (bkpts 2 &4) • RT-PCR using F primer in exon 49 of dystrophin showed: • 658 bp product comprising 3’ end of ex 49 spliced to exs 50 & 51, followed by 215 bp of int 51 and then consensus AUUAAA polyadenylation signal
Phenotype • Muscular dystrophy, high CKs - single exon deletion & partial inversion of dystrophin gene • Glycerol kinase deficiency – deletion of GK gene • Congenital adrenal hypoplasia – NROB1 (DAX1) gene deleted • Learning difficulties associated with mutations in IL1RAPL1 gene
Origin of mutation - linkage studies • QF-PCR showed RD’s mother, CMD, to be a carrier of the ex52 del (and therefore of the Xp21 rearrangement). • CMD has inherited the high risk X from her father, PD. • PD not affected, therefore de novo mutation in CMD or PD is germline mosaic for inversion.
4 1 3 2 4 2:4 2 1:3 4:2 1 3 3:1 2:4 1:3 3:1 4:2 Mutational mechanism
Detection of inversions • At the time (2001), this inversion would not have been detected using our regular DMD testing strategy (karyotype & QF-PCR) – only investigated further as doctors noted DMD, GKD, CAH etc and patient diagnosed with contiguous gene disorder. • Much of this work wouldn’t be necessary if referred now – this rearrangement detectable by arrays. • BUT only detectable as is complex with deletion as well as inversion:
High density aCGH Inversion of exs 53 to 79 of dystrophin Dystrophin IL1RAPL1 +7 +6 +5 +4 +3 +2 +1 0 -1 -2 -3 -4 -5 -6 -7 Deletion of dystrophin exon 52 Deletion including 11 genes
Reference & acknowledgements • A complex deletion-inversion-deletion event results in a chimeric IL1RAPL1-dystrophin transcript and a contiguous gene deletion syndrome. Wheway et al, JMG (2003); 40: 127-131 • Lab work carried out by: • Jo McCauley (Wheway) • Michael Yau • Vandana Nihalani • David Ellis • Vicky Cloke