Download
1 / 26
260 likes | 360 Views
Sullivan County Regional Health Council Overview. Stephen May November 15, 2011. Health Council Composition . Approximately 30 members of the community Cross all spectrums: Business and Industry, Hospitals, Private Health Care Providers, Religious, Insurance providers,

E N D
Sullivan County Regional Health Council Overview Stephen May November 15, 2011
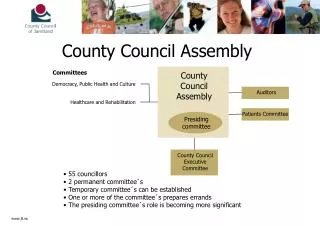
Health Council Composition • Approximately 30 members of the community • Cross all spectrums: Business and Industry, Hospitals, Private Health Care Providers, Religious, Insurance providers, • Health department provides support, program structure, epidemiology. • CDC MAPP Model (Mobilizing for Action through Planning and Partnerships)
Our Vision and Value Statements Vision: A safe, healthy, and educated Sullivan County. Value Statements: ~Education:We value community health education. ~Access:We value access to community resources. ~Collaboration:We value partnerships and collaborative efforts. ~Compassionate Commitment:We value a caring holistic approach to community health. ~Culture:We value the various cultures and the diversity they bring to our community ~ Accountability:We value a commitment from both individuals and the community to take ownership for a healthier Sullivan County.
MAPP Principals • The following principals are integral to the successful implementation of MAPP: • Systems thinking — to promote an appreciation for the dynamic interrelationship of all components of the local health system required to develop a vision of a healthy community. • Dialogue — to ensure respect for diverse voices and perspectives during the collaborative process. • Shared vision — to form the foundation for building a healthy future. • Data — to provide factual information during each step of the process. • Partnerships and collaboration — to optimize performance through shared resources and responsibility. • Strategic thinking — to foster a proactive response to the issues and opportunities facing the system. • Celebration of successes — to ensure that contributions are recognized and to sustain excitement for the process
4 MAPP Assessments • Community Themes and Strengths • Local Public Health System • Forces of Change • Community Health Status
Community Health Status Data Sources: • Death 1990 – 2004 added 2005-2006 • Hospitalizations (Outpatient and Inpatient ) Outpatient 1998 - 2004 Inpatient 1997 – 2004 • Infectious Disease – Tennessee Dept of Health • Census 2000 and American Community Survey • Births – Teen pregnancy • Behavioral Risk Factor Surveillance Survey 2005
Matrix Weighting and Scoring • Percent deaths • Percent Hosp ER • Percent Hospital Inpatient • Severity of Consequences • Trends • High incidence or prevalence • Healthy People 2010 • Instate priority • Acceptability to citizens
Disease Diagrams • Literature Searches for each health outcome • Identified: Precursors Consequences Linkages • Health Council Members localized diagrams
Tallied Risk Factors + Consequences 5 risk factors affected all 28 diseases • Less than High School Education • Lack of Resources/Poverty • Access Barriers (lack of health insurance, lack of transportation, absence of childcare, etc) • Limited Employment Opportunities • Health Literacy/Hygiene Knowledge + Practice
Community Themes & Strengths Assessment • Convenience Sample Survey – captures thoughts of individual citizen - public libraries, grocery stores, malls, beauty salons • Produced a ranking of the top 15 causes
Forces of Change Assessment • 2 Focus Group sessions consisting of community leaders: - legislators, police, local government, non-profit health care agencies, schools, United Way, various agencies representing child + youth services, individual citizens • Goal was to identify forces and/or themes in the community that has or would cause an affect on the health of Sullivan County citizens • Discussions were guided around topics of politics, environment, technology, socio-cultural changes and legal
Top Issues: Focus Group Assessment • Lack of Affordable, safe housing • Poor Air Quality • Steady use of fast food restaurants • Sub-optimal level of prenatal education for teens • Sub-optimal level of high school completion rate relating to lack of educated workforce • Lack of political lobbying: local and state level • Increased drug use • Increase in family violence • Increase in depression • Aging Population
Local Public Health System Assessment • Evaluated Sullivan County’s total health system is doing in providing the 10 Essential Public Health Services as identified by the CDC • 5 areas surfaced as being areas with opportunity for improvement
Local Public Health System Assessment’s Areas with Opportunity for Improvement • #3 Inform, educate and empower people about health issues • #5 Develop policies and plans that support individual and community efforts • #6 Enforce laws and regulations that protect health and ensure safety
All together, what do the 4 assessments say? • All 4 assessments offered a consistent list of the top causes of health concerns and precursors within Sullivan County • 2 important disease precursors surfaced from all 4 assessments': - Less than a high school education - Lack of political lobbying: local and state level
Phase 1 Results • Data Summary Reference • Compilation of common risk factors • Resource utilization, morbidity, mortality matrix • Preliminary rankings of diseases with most impact on community.
Overview Phase 2Expanded Structure • HC is transitioning… • from planning to operational phase • MAPP Builds local health leadership, but also promotes community responsibility for the health of the public • Steps to Success • Community-driven HC • Strategic planning and evaluation from HC • Engaging community partners (external to HC)
OverviewExpanded Structure Recommendations • Preparing for Action Cycle • Evaluate – Plan – Implement • Based on HC best practices: • Establish Steering Group (HC) • Establish Health Priority Task Forces &Workgroups • Goal: Engagement of Community Partners • Expand operational structure for “implement”
Steering Group(Proposed) • Purpose: • Strategic direction for HC & MAPP • Planning for short term • (e.g., HC meeting objectives and agendas) • Planning for long term • (e.g., annual goals for MAPP) • Membership: • 3 HC members + HC Coordinator (SCRHD) • Advisor: Dr. May (SCRHD) • Frequency: • Meet 1-2 weeks after each HC mtg
Task Force Logic Model Steps • Why is the disease a problem? Target groups? • Who are our stakeholders and partners? • What processes or programs currently exist? • What are the best practices and best programs in other areas? • Bench marking • Gap analysis • Design Custom community action plan to target issue. • Design appropriate measures for program • Measure results • Plan, do, check, act cycle
Community Partners • Healing Hands and Friends in Need • REACH • CHIP – more regional • Project Access • NE TN Regional Health Council • TN Dept of Health and CDC