Download
1 / 1
10 likes | 145 Views
Hypothesis. Materials and Methods. Results. Conclusions. Low risk. Low risk. Low risk. High risk. High risk. High risk.

E N D
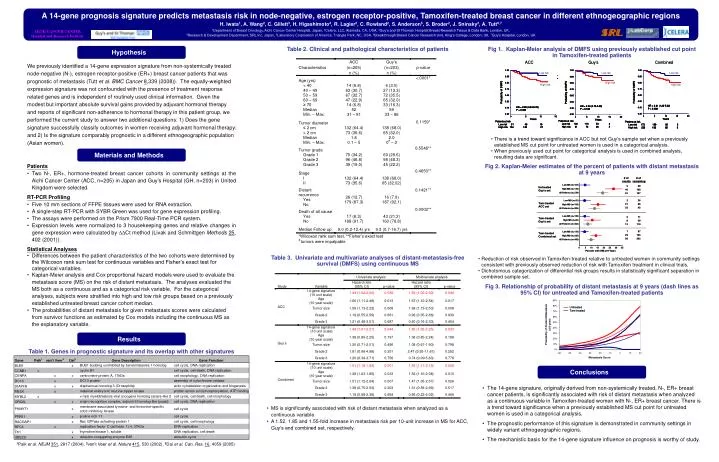
Hypothesis Materials and Methods Results Conclusions Low risk Low risk Low risk High risk High risk High risk A 14-gene prognosis signature predicts metastasis risk in node-negative, estrogen receptor-positive, Tamoxifen-treated breast cancer in different ethnogeographic regions H. Iwata1, A. Wang2, C. Gillett3, H. Higashimoto4, R. Lagier2, C. Rowland2, S. Anderson5, S. Broder2, J. Sninsky2, A. Tutt6,71Department of Breast Oncology, Aichi Cancer Center Hospital, Japan, 2Celera, LLC, Alameda, CA, USA, 3Guy’s and St Thomas’ Hospital Breast Research Tissue & Data Bank, London, UK, 4Research & Development Department, SRL Inc, Japan, 5Laboratory Corporation of America, Triangle Park, NC, USA, 6Breakthrough Breast Cancer Research Unit, King’s College, London, UK, 7Guy’s Hospital, London, UK Table 2. Clinical and pathological characteristics of patients Fig 1. Kaplan-Meier analysis of DMFS using previously established cut point in Tamoxifen-treated patients We previously identified a 14-gene expression signature from non-systemically treated node-negative (N-), estrogen receptor-positive (ER+) breast cancer patients that was prognostic of metastasis (Tutt et al. BMC Cancer8,339 (2008)). The equally-weighted expression signature was not confounded with the presence of treatment response related genes and is independent of routinely used clinical information. Given the modest but important absolute survival gains provided by adjuvant hormonal therapy and reports of significant non-adherence to hormonal therapy in this patient group, we performed the current study to answer two additional questions: 1) Does the gene signature successfully classify outcomes in women receiving adjuvant hormonal therapy; and 2) Is the signature comparably prognostic in a different ethnogeographic population (Asian women). • There is a trend toward significance in ACC but not Guy’s sample set when a previously established MS cut point for untreated women is used in a categorical analysis. • When previously used cut point for categorical analysis is used in combined analysis, resulting data are significant. • Patients • Two N-, ER+, hormone-treated breast cancer cohorts in community settings at the Aichi Cancer Center (ACC, n=205) in Japan and Guy’s Hospital (GH, n=203) in United Kingdom were selected. • RT-PCR Profiling • Five 10 mm sections of FFPE tissues were used for RNA extraction. • A single-step RT-PCR with SYBR Green was used for gene expression profiling. • The assays were performed on the Prism 7900 Real-Time PCR system. • Expression levels were normalized to 3 housekeeping genes and relative changes in gene expression were calculated by DDCt method (Livak and Schmittgen Methods25, 402 (2001)). • Statistical Analyses • Differences between the patient characteristics of the two cohorts were determined by the Wilcoxon rank sum test for continuous variables and Fisher’s exact test for categorical variables. • Kaplan-Meier analysis and Cox proportional hazard models were used to evaluate the metastasis score (MS) on the risk of distant metastasis. The analyses evaluated the MS both as a continuous and as a categorical risk variable. For the categorical analyses, subjects were stratified into high and low risk groups based on a previously established untreated breast cancer cohort median. • The probabilities of distant metastasis for given metastasis scores were calculated from survivor functions as estimated by Cox models including the continuous MS as the explanatory variable. Fig 2. Kaplan-Meier estimates of the percent of patients with distant metastasis at 9 years Table 3. Univariate and multivariate analyses of distant-metastasis-free survival (DMFS) using continuous MS • Reduction of risk observed in Tamoxifen-treated relative to untreated women in community settings consistent with previously observed reduction of risk with Tamoxifen treatment in clinical trials. • Dichotomous categorization of differential risk groups results in statistically significant separation in combined sample set. Fig 3. Relationship of probability of distant metastasis at 9 years (dash lines as 95% CI) for untreated and Tamoxifen-treated patients Table 1. Genes in prognostic signature and its overlap with other signatures • The 14-gene signature, originally derived from non-systemically treated, N-, ER+ breast cancer patients, is significantly associated with risk of distant metastasis when analyzed as a continuous variable in Tamoxifen-treated women with N-, ER+ breast cancer. There is a trend toward significance when a previously established MS cut point for untreated women is used in a categorical analysis. • The prognostic performance of this signature is demonstrated in community settings in widely variant ethnogeographic regions. • The mechanistic basis for the 14-gene signature influence on prognosis is worthy of study. • MS is significantly associated with risk of distant metastasis when analyzed as a continuous variable • A 1.52, 1.85 and 1.55-fold increase in metastasis risk per 10-unit increase in MS for ACC, Guy’s and combined set, respectively. 1Paik et al. NEJM351, 2817 (2004), 2van’t Veer et al. Nature415, 530 (2002), 3Dai et al. Can. Res.16, 4059 (2005)