Download
1 / 16
180 likes | 452 Views
Acute Heart Failure in Apical Ballooning Syndrome (Takotsubo/Stress Cardiomyopathy) Clinical Correlates and Mayo Clinic Risk Score. Malini Madhavan, MBBS; Charanjit S. Rihal, MD, FACC; Amir Lerman MD, FACC; Abhiram Prasad, MD, FRCP, FACC Division of Cardiovascular Diseases

E N D
Acute Heart Failure in Apical Ballooning Syndrome (Takotsubo/Stress Cardiomyopathy)Clinical Correlates and Mayo Clinic Risk Score Malini Madhavan, MBBS; Charanjit S. Rihal, MD, FACC; Amir Lerman MD, FACC; Abhiram Prasad, MD, FRCP, FACC Division of Cardiovascular Diseases Mayo Clinic, Rochester No relevant author disclosures J. Am. Coll. Cardiol. 2011;57;1400-1401
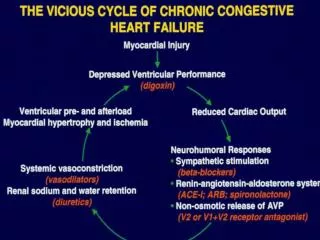
Background • Apical ballooning syndrome (ABS) is characterized by transient regional systolic dysfunction of the left ventricle in the absence of obstructive coronary artery disease • Acute heart failure (HF) is the most common complication • Acute HF can cause significant morbidity in ABS
Aims • To examine the frequency and prognosis of patients with acute HF complicating ABS • To identify the risk factors for acute HF in ABS
MethodsStudy Population • Study cohort • 118 consecutive ABS patients identified between January 2002 and January 2008 • Validation cohort • 52 consecutive ABS patients identified between Feb 2008 and December 2009
MethodsMayo diagnostic criteria for ABS • Transient akinesis, hypokinesis or dyskinesis of the left ventricular mid segments with or without apical involvement. The regional wall motion abnormalities extend beyond a single epicardial vascular distribution • Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture, • New ECG abnormalities (either ST-segment elevation and/or T wave inversion) or elevated cardiac troponin, • The absence of pheochromocytoma or myocarditis Prasad et al. Am Heart J 155(3):408-17
Methods: Definitions Acute heart failure • New onset symptoms such as dyspnea, and • At least 2 of the following physical signs - pulmonary rales, elevated central venous pressure, and the presence of a third heart sound Cardiogenic shock • Systolic blood pressure of <90 mm Hg for greater than 1 hour secondary to cardiac dysfunction associated with signs of hypoperfusion • Patients with systolic blood pressure increase to >90 mm Hg within 1 hour after administration of inotropic agents, who met other criteria for cardiogenic shock
Independent Predictors of Acute HFMultivariate Analysis *Per unit change in variable
Mayo Clinic Risk Score for Acute HF in ABS • One point was assigned to each of the following independent risk factors: • Age > 70 years • Presence of physical stressor • Ejection fraction < 40% • Troponin T was not included due to heterogeneity in assay and cut-off value used at different institutions
Mayo Clinic Risk Score for Acute HF in ABS • Significant positive correlation between the frequency of acute HF and the risk score in the: • Development cohort – C statistic 0.77, p<0.001 • Validation cohort – C statistic 0.77, p=0.002
Acute HF Stratified by Mayo Risk Score Development cohort Validation cohort
Conclusions • Heart Failure is a common complication of ABS • Approximately 50% developed HF • One in five developed cardiogenic shock • Patients who developed acute HF had, • Greater myocardial injury and stunning • Greater morbidity and longer hospitalization • Prognosis is good with resolution of HF with supportive management in the majority of patients • Mortality secondary to cardiogenic shock occurred in 3 patients
Conclusions • The Mayo Clinic risk score is predictive of acute HF in patients with ABS • Risk stratification using the Mayo Clinic risk score may: • Assist in triaging high risk patients to an intensive care unit for management • Allow physicians to identify patients in whom early initiation of beta-adrenergic blockers may be harmful