Download
1 / 28
280 likes | 707 Views
The Dizzy Patient: An Introduction. If someone says that he can think or talk about quantum physics without becoming dizzy, that shows only that he has not understood anything whatever about it. Murray Gell-Mann.

E N D
The Dizzy Patient: An Introduction If someone says that he can think or talk about quantum physics without becoming dizzy, that shows only that he has not understood anything whatever about it. Murray Gell-Mann
A 62 year old man is evaluated for a 2-week history of dizzyness. Episodes of dizzyness occur several times per day, usually in the morning and at bedtime, and typically last about 15 to 30 seconds, particularly when he rolls over in bed. The dizzyness is described as a spinning sensation and is associated with mild nausea but not vomiting. He has one previous episode of dizziness at the age of 28 years for which he went to the emergency department and received meclizine; that episode resolved in 3 days. The patient has hypertension and DMII and his current medications are HCTZ and glipizide. On physical exam, supine pulse rate and blood pressure are 72/min and 120/80mmHg, and values on standing are 76/min and 116/84mmHg, The Hallpike manuever results in dizzyness and mild nystagmus when the patient is recumbent with the left ear down but not with the right ear down. There are no focal neurological findings and the remainder of the exam is normal. Which of the following is the most appropriate for managing this patient’s disorder?A) CT Scan of HeadB) ElectronystagmographyC) MeclizineD) Habituation exercisesE) Decreased HCTZ dose
Antonio Tiger is an 72 y.o. African American male patient with Hx of gout, CVA 1996, HTN, DMII, PE treated with coumadin who presents to the ED with complaint of feeling lightheaded and almost passing out in the waiting line of clinic. He admits to standing in line at CamCare for 1.5 hours feeling jittery and needing to rely more on his cane of his right hand to support his weight. He sat down once and felt better and attempted to stand in line again. This time he fell into a wall, with his left shoulder, did not hit his head, had not hit his head recently and slumped to the floor where he was assisted by other patients. He denies LOC, seizure like activity, tongue biting or loss of bowel or bladder control. Patient checks his sugars at home each morning at his sugars have been running 200 to 150s and never lower than 80. Only checks in the AM. Admits to eating only 1 bowel of cereal this AM, not eating lunch today. Denies nausea, diaphoresis, SOB, CP nor palpitations. He has been able to walk around a football field and has done some often in the last several weeks.Denies recent diarrhea, has good po intake except this AM and takes his medications regularly.
Pre-syncope -a feeling of losing consciousness or blacking outOne of the most common causes of pre-syncope is orthostatic hypotension. Blood pressure and cerebral perfusion is maintained by several physiological mechanisms: Upon standing 300-800cc of blood pooling occurs and an appropriate compensatory mechanism requires the coordination of several systems: There must be a sufficient excessive amount of reserve blood to compensate for the transitory loss of that 300-800cc. Diuretics, sepsis, hypovolemia from any etiology could drain any venous reserve that would be mobilized.
muscle contraction of abdominal and leg muscles contract and squeeze anatomically placed venous reservoirs back towards the heart. The veins have one way valves that coordinate movement into blood return. Thus patients with impaired venous return or damaged venous valves will be unable to effectively mobilize the force generated from the muscle contraction. Also in a patient standing for an extended period of time without movement, there is insufficient movement to continue to recycle blood up from the venous reservoir.
The carotid and aortic baroreceptors sense the decrease of perfusion and send a sympathetic feedback to the heart, arteries and veins. • Diabetic neuropathy, Guillain-Barre, Vasovagal, Alcohol, HIV, Syphilis, Multiple Sclerosis can all induce autonomic neuropathy.
The heart to increase heart rate and cardiac contractility, the arteries to contract to increase Total peripheral resistance and Mean Arterial Pressure. In patients with cardiomyopathy, myocardial infarction, pericardial effusion, pericarditis, arrythmias that compromise cardiac output may prevent appropriate cardiac compensation. Beta blockers and CCB could contribute to this.
There must be a sufficient excessive amount of reserve blood to compensate for the transitory loss of that 300-800cc. Diuretics, sepsis, hypovolemia from any etiology, post-prandial effects, could drain any venous reserve that would be mobilized.
Orthostatic Hypotension Associated Medications • doxazosin, terazosin, (alpha-blockers) • Carvedilol, labetalol, • Ace-inhibitors, Clonidine, • Dipyridamole, • Furosemide, Hydralazine, • Methydopa, • Nitrates, • Reserpine, • Chlorpromazine, • clozapine, • opioids, • bromocriptine, levadopa/carvidopa, • baclofen, cyclobenzaprine, • methocarbamol, • Amitriptyline (TCA) • sildenafil (Phosphodiesterase type 5 inhibitors), • oxybutynin (urinary anticholinergics) Alcohol insulin
Treatment for Orthostatic Hypotension: • Stop offending medications, fluids • Fludrocortisone: 0.1mg/day • Midodrine 30mg/day • Indomethacin (prostaglandin inhibitor) • Caffeine
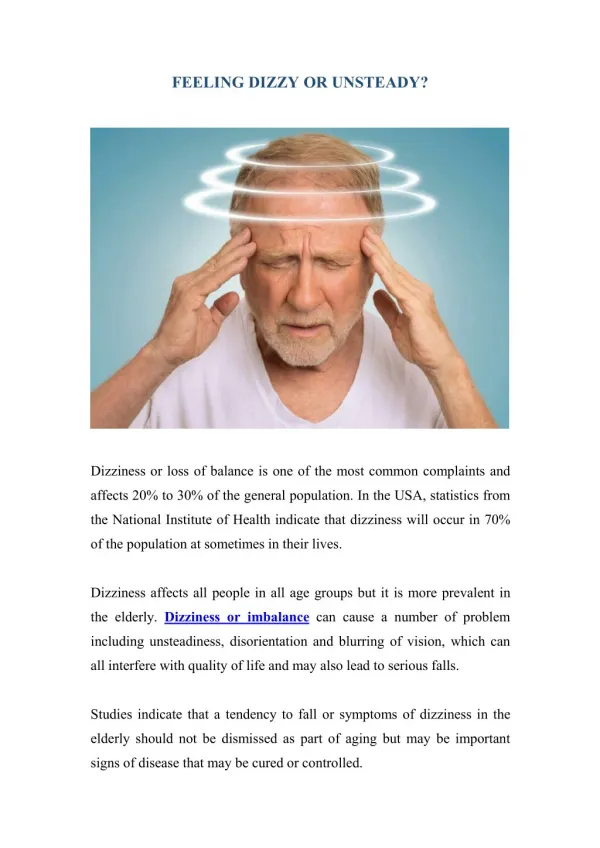
There are four major categories of Dizzyness Vertigo Disequilibrium Presyncope Lightheadedness
Vertigo- the sensation of motion when there is no motion relative to Earth’s gravity. It has both benign and alarming etiologies. Benign Paroxysmal Positional Vertigo-loose otolith in semicircular canal resulting in positional episodes of vertigo, diagnosed with Dix-Hall Pike, and can be treated with Epley manuever and vestibular habituation exercise. Vestibular Neuritis-peripheral vertigo secondary to viral infection and inflammation of vestibular nerve, with selective damage to superior vestibular labyrinth, producing vertigo, spontaneous nystagmus, positive head thrust, imbalance towards affected side, and N/V diaphoresis, could be treated with methyprednisolone and vestibular exercises. Labyrinthitis- peripheral vestibulopathy from prodromal viral illness or adjacent bacterial spread with acute vertigo onset over several hours peaking at 24 hours and resolving over up to months later, associated hearing loss, spontaneous nystagmus, vomiting. Treat with Methprednisolone and meclizine/scopolamine, as well as vestibular rehab. Meniere disease- unknown etiology, a syndrome of acute onset vertigo, low frequency hearing loss unilaterally and tinnitis, with spontaneous nystagmus on exam, can treat with meclizine/scopolamine, and HCTZ/acetazolamide, salt restriction and caffeine abstinence. Migrainous vertigo- diagnose with concommitent photophobia, aura, phonophobia and headache, treat as with regular migraine, in patient with known migraine history. Ramsey Hunt Syndrome- Herpes Zoster infection of the 7th CN and geniculate ganglion, resulting in hearing loss, vertigo and facial nerve palsy. Treat with prednisone and acyclovir.
Tumors of cerebellopontine angle-presents with tinnitis, then vertigo, hearing loss and facial palsies. Nystagmus vertical and non-fatigable. • Cerebellar stroke- ischemic stroke that presents with vertigo, gait instability, secondary to acute infarct of posterior fossa, diagnosed with MRI. • Vertebrobasilar stroke- ischemic stroke secondary to compromise of some portion of the vertebral basilar arterial distribution, presenting with vertigo, headache, confusion, pupillary abnormalities, facial palsy, hemiplegia or quadraplegia, best diagnosed with MRI and then treated via stroke protocol.
Vertigo can be central or peripheral in terms of lesion location Central- vestibular nuclear complex, vertivulocerebellum, braintem, spinal cord and vestibular cortex Peripheral-vestibular nerve, otoliths, and semicircular canal.
Central and peripheral can be distinguished by History and PE • Central- chronic over course of weeks to months, may be exacerbated by movement, associated with non- fatigable vertical nystagmus. Vertigo can be associated with facial and auditory nerve palsies, and visual field abnormalities. • Rhomberg, Finger-Nose and pronator drift abnormalities all indicate cerebellar and thus a central lesion.
Central and peripheral can be distinguished by History and PE • Peripheral- the vertigo is sudden and severe, brought on by sudden head movements, relieved with absolute head stillness, lasts seconds to minutes, often associated with ear fullness, tinnitis, nausea and vomiting. Associated with horizonal nystagmus that is fatigable.
Diagnostic Tests • Head Thrust- asking the vertiginous patient to focus on your nose, (after warning them) swivel their neck right to left rapidly, 30 degree (but with great care), and focus on their eyes. • IF the patient is unable to track your nose effectively, I.e. they look beyond it and then recollect on the nose, you can be fairly certain that the patient’s VOR (vestibular ocular reflex is compromised) This means that the lesion that is inducing the vertigo is likely peripheral
IF the eyes follow the nose carefully, even in the setting of acute vertigo, then your patient may have a crebellar infarct that is allowing the Vestibular ocular reflex to bypass the cerebellum. • In these patients it is prudent to be concerned for Cerebellar infarct, and if able an MRI brain>CT head is warrented. • This is because CT head is a poorer study for posterior cranial fossa lesions
Of note: 75% of all cerebellar strokes present with vertigo (often in conjunction with nausea, vomiting, headache and gait instability), but only 1% of cerebellar stroke present with just vertigo.
Diagnostic Tests Orthostatic Blood Pressure- Orthostatic hypotension is a physical finding defined by the American Autonomic Society and the American Academy of Neurology as a systolic blood pressure decrease of at least 20 mm Hg or a diastolic blood pressure decrease of at least 10 mm Hg within three minutes of standing.
Diagnostic Tests Orthostatic Blood Pressure- Orthostatic hypotension is a physical finding defined by the American Autonomic Society and the American Academy of Neurology as a systolic blood pressure decrease of at least 20 mm Hg or a diastolic blood pressure decrease of at least 10 mm Hg within three minutes of standing. In some articles, it is within one minute, and the recommended rate of pulse increase was 30bpm over the sitting value.
Dix-HallPike Maneuver • Dix-Hallpike test for BPPV. A person is brought from sitting to a supine position, with the head turned 45 degrees to one side and extended about 20 degrees backward. Once supine, the eyes are typically observed for about 30 seconds. If no nystagmus ensues, the person is brought back to sitting. There is a delay of about 30 seconds again, and then the other side is tested. A positive Dix-Hallpike tests consists of a burst of nystagmus.
Epley Maneuver • 1. Sit upright. • 2. Turn your head to the symptomatic side at a 45 degree angle, and lie on your back. • 3. Remain up to 5 minutes in this position. • 4. Turn your head 90 degrees to the other side. • 5. Remain up to 5 minutes in this position. • 6. Roll your body onto your side in the direction you are facing; now you are pointing your head nose down. • 7. Remain up to 5 minutes in this position. • 8. Go back to the sitting position and remain up to 30 seconds in this position. • The entire procedure should be repeated two more times, for a total of three times. • During every step of this procedure the patient may experience some dizziness.
Laboratory Workup “Because they generally are not helpful diagnostically, laboratory testing and radiography are not routinely indicated in the workup of patients with dizzyness when no other neurologic abnormalities are present.” American Association of Family Practice
Vestibular Exercises • Vestibular Exercise Program to Overcome Dizziness • AIMS OF EXERCISE • 1. To loosen up the muscles of the neck and shoulders, to overcome the protective muscular spasm and the tendency to move “in one piece.” • 2. To train movement of the eyes, independent of the head. • 3. To practice balancing in everyday situations with special attention to developing the use of the eyes and the muscle senses. • 4. To practice head movements that cause dizziness, and thus gradually overcome the disability. • 5. To become accustomed to moving about naturally in daylight and in the dark. • 6. To encourage the restoration of self-confidence and easy spontaneous movement. • http://drnguyen.ucsd.edu/Default.aspx?tabid=77
Cawthorne’s Head Exercises • Exercises are to be carried out for 15 minutes twice a day, increasing to 30 minutes. • EYE EXERCISES • Look up, then down – at first slowly, then quickly, 20 times. • Look from one side to the other – at first slowly, then quickly, 20, times. • Focus on your thumb at arm’s length, moving it one foot toward you and back again, 20 times. • HEAD EXERCISES • Bend head forward then backward with eyes open – slowly, later quickly, 20 times. • Turn shoulders to right, then to left, 20 times. • Bend forward and pick up objects from the ground and sit up 20 times. • STANDING • Change from sitting to standing and back again, 20 times with eyes open. Repeat with eyes closed. • Throw a small rubber ball from hand to hand above eye level. Throw ball from hand to hand under one knee. • MOVING ABOUT • Walk across the room with eyes open, then closed, 10 times. • Walk up and down a slope with eyes open, then closed, 10 times. • Walk up and down steps with eyes open, then closed, 10 times. • Any game involving stooping or turning is good.
References Kulstad, C. and Hannafin B. Dizzy and Confused: A Step-by-Step Evaluation of the Clinician's Favorite Chief Complaint, Emergency Medicine Clinics of North America: Volume 28, Issue 3, August 2010, Pages 453-469 Post, R. and Dickerson, L. Dizziness: A Diagnostic Approach, American Family Physician: Volume 82, Number 4, August 15, 2010 BRADLEY J., and DAVIS K., Orthostatic Hypotension Am Family Physician. 2003 Dec 15;68(12):2393-2399 Ferri, F. Ferri’s Clinical Advisor: Instant Diagnosis and Treatment. Mosby-Elsevier, USA, 2007. http://drnguyen.ucsd.edu/Default.aspx?tabid=77: Official Website of the University of California at San Diego, School of Medicine