Download
1 / 52
530 likes | 849 Views
Dr. Roman Jaeschke Dr. Mark Soth Lily Waugh Members of the CCRT. A Celebration of Team Work at SJHH Enticing the Hospital to Join Your Team C ritical C are R esponse T eam. We Gratefully! Acknowledge Team members of CCRT - St. Joseph’s Healthcare Hamilton

E N D
Dr. Roman Jaeschke Dr. Mark Soth Lily Waugh Members of the CCRT A Celebration of Team Work at SJHHEnticing the Hospital to Join Your TeamCriticalCareResponseTeam
We Gratefully! Acknowledge Team members of CCRT - St. Joseph’s Healthcare Hamilton Staff of St. Joseph’s Healthcare Hamilton Deanna Burnet Linda Gandy Julie Garnham-Takaoka Ann Higgins Neala Hoad Margaret Maclennan Dr. Dan Perri Tracy Watson MOHLTC - Critical Care Secretariat Provincial and LHIN Colleagues Sisters of St. Joseph’s for their Legacy THANK YOU!
We will present: The Who, What, and How of the CCRT CCRT - Jeopardy CCRT - Interactive Scenarios
Everyone experiences teams and team work in a different manner. Each team member has their own expectations and assumptions about team work. The quality of team relationships is key to positive patient and staff safety outcomes. Our day to day interactions play a significant role in patient satisfaction and the quality of our work life. Each team member has the potential to add to a positive experience of team work. Common goals and values enhance the team. The SJHH Mission Excellence model reflects common team goals and values. Value of Teamwork
The system opportunities are becoming increasingly recognized Institute for HealthCare Improvement
Deployment of Rapid Response Teams (CCRT) √ Reliable, Evidence-Based Care for AMI Medication reconciliation Prevention of Central Line Infections Prevention of Surgical Site Infections Prevention of VAP Six Changes That Save Lives
MOHLTC has established the Critical Care Secretariat under leadership of Dr. Bernard Lawless Ontario’s Critical Care StrategySeven Components to achieve 3 goals 1. CCRT Expansion 2. System -Level Training Initiatives 3. Critical Care Information System 4. Coaching Teams / LHIN Leaders 5. Ethical Issues of Access 6. HHR Investments 7. ICU Capacity Investments Improve Access Improve Quality Work As A System
The Ontario Critical Care Strategy is designed to improve access, quality and system integration in the provisions of critical care services. Critical Care Response Teams (CCRT) have the potential to significantly impact adult critical care resources by bringing specialist knowledge and skills from the Intensive Care Unit (ICU) as needed, directly to the bedside 24/7. Ontario Critical Care Strategy & CCRT • Critical Care Response Teams are also referred to as: • ACCESS • Outreach • Rapid Response Team (RRT) • Medical Emergency Team (MET) • Rapid Assessment of Critical Events • (RACE)
Team of clinicians who bring critical care expertise to the patient’s bedside or wherever it is needed. CCRT goals include: Patient and staff safety Early identification and intervention for patients at risk of deterioration Obtain help before there is an emergency Extending the specific ICU skillsbeyond the ICU walls Enable more timely ICU admission and decreased LOS Facilitate teamwork, knowledge transfer and mutual collaboration of patient goals and plan of care What is a CCRT ?
Role of CCRT ICU admission Ward patient Timely referral Discharge to ward Deterioration ICU admission prevented Follow-up on ward Early intervention Deterioration Safe discharge home Scales and Sibbald, Critical Care Rounds 2002
Phase 1- May to October 2006 CCRT recruitment and education Phase 2 - November to January 2007 CCRT Preceptorship CCRT available Monday-Friday from 08:00 - 16:00 Phase 3 - January 29, 2007 24/7 CCRT coverage
“We will build the team as we go”. Dr. Roman Jaeschke, 2006, CCRT Implementation
CCRT Team Model Members • Physicians with Critical Care training and experience • Experienced Critical Care trained Nurses • Experienced Respiratory Therapists • Ward Staff • MRP - attending MD and MRP house staff
Work collaboratively with hospital ward staff to identify, assess and respond to the needs of patients To assist the MRP team not to replace Providing early and timely patient intervention Expand Critical Care skills beyond the walls of ICU Provide Critical Care skills where they are needed A Team supporting a Team Team Model
For CCRT to work…. Patient must manifest warning signs Educate & Heighten Awareness Empower front-line staff “Protected” Response Staff Critical Care MD’s, RNs, RTs Help must be called for Help must arrive Help must have appropriate skill set How was this process working before CCRT? Has CCRT changed it ?
Retrospective chart review Jan 01, 2005 until June 30, 2005 Unplanned ICU admissions or Code Blue Patients from the OR, ED, and outpatients were excluded 164 unplanned ICU admissions plus 19 Code Blue patients that did not survive to ICU Post - CCRT Implementation Prospectively collected data by CCRT RN for MOH More detailed retrospective chart review Feb1, 2007 to July 31, 2007 (1st 6 mths. CCRT) 93 unplanned admissions and 4 Code Blue patients that did not survive to ICU Pre - CCRT Implementation
Do Patients Manifest Signs of Trouble Prior to Admit/Code?
How Long Do Patients Manifest Signs of Trouble Prior to Admit/Code?
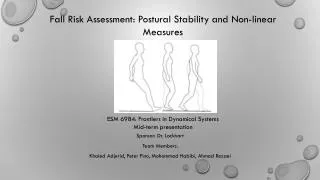
How long before the MD is paged?Has this improved post CCRT? Post-CCRT Pre-CCRT
How long before the MD is paged?Has this improved post CCRT? p=0.002
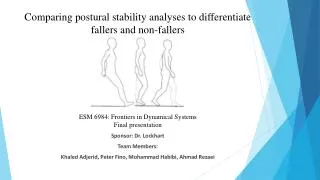
How long before the MD responds (Code Blues Excluded)? Post-CCRT Pre-CCRT
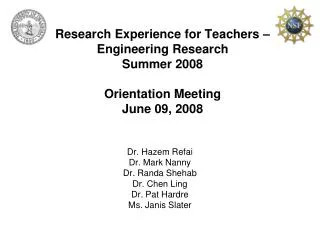
Who is the MD first responder?Has this changed post CCRT? Post-CCRT Pre-CCRT CCRT did not displace the MRP physician team
Did CCRT work…. Yes – 84% manifest signs & over half for >8h Yes – the common signs are CCRT criteria Patient must manifest warning signs Help must be called for Help must arrive Help must have appropriate skill set
Did CCRT work…. Patient must manifest warning signs Yes – Significance of signs recognized and staff empowered to notify MD earlier Help must be called for Help must arrive Help must have appropriate skill set
Did CCRT work…. Patient must manifest warning signs Help must be called for Yes & No – No change in resident response time Yes – Slight increase in MRP attending response Yes – Major increase in critical care attending RN, & RT response Help must arrive Help must have appropriate skill set
Did CCRT work…. Yes – 84% manifest signs & over half for >8h Yes – the common signs are CCRT criteria Patient must manifest warning signs Yes – Significance of signs recognized and staff empowered to notify MD earlier Help must be called for Yes & No – No change in resident response time Yes – Slight increase in MRP attending response Yes – Major increase in critical care attending, RN, & RT response Help must arrive Help must have appropriate skill set
32 year old female with Crohn’s disease, on steroids To ER ~ midnight. Referred to GI with abdominal pain System problem (ER responsibility, GI availibility) GI resident ~ 11 am, CCRT called almost immediately HR 140, Temp 39, SBP 80, lactate 6, no urine output System problem (too sick for ER) CCRT RN, cooperation, rapid resuscitation, Abx ICU status - 22 ventilated patients in 15 bed ICU. No ICU beds Patient to CCU System problem (too sick for CCU) CCRT RN, cooperation, resuscitation, satisfaction Surgical consult System problem (most junior person first) Calling in staff surgeon, rapid resuscitation What makes CCRT worthwhile? We think…
Patient in the OR at 15:00 Patient ventilated in PACU as ICU overflow - Managed in PACU by ICU as 7th ICU overflow patient Patient transferred to Surgical Stepdown next day Patient transferred out of Surgical Stepdown the following day What makes CCRT worthwhile? We know…
Less ICU admissions? Decrease in ICU overflow? Lower mortality? Lower cardiac arrest rate? How do we measure CCRT success?
“Culture to an institution is like personality is to an individual”. Dr. Deborah Cook, 2008, Legacy
Patient at the center of care Service Excellence (C.A.R.E.) C ompassion A ttitude R esponsiveness E xcellence Other Outcomes… Mission Excellence
Pre-CCRT Implementation Survey 82 ward staff respondents… I am able to obtain assistance from a physician in a timely manner….
Staff and Physician collaboration Providing increased Physician and Medical Learner support Empowerment of CCRT RN and RT Leadership development Ambassadors of Critical Care Empowerment of Ward Staff It is ok to call for help Exceeding patients and each others’ expectations Develop future interest in Critical Care Other Outcomes… Quality of Work-Life
Post-CCRT Implementation Post CCRT Referral Survey Knowing the CCRT is available makes caring for very sick people less stressful…. Quality of Work Life
Post-CCRT Implementation Post CCRT Referral Survey I am comfortable initiating a call to the CCRT…. Staff Empowerment
Other Outcomes… Patient Safety • Patient Safety is an identified priority and key strategic goal • of St. Joseph's HealthCare, Hamilton (SJHH) • A culture of safety has been established within the hospital • through several corporate initiatives, one of which is the • Critical Care Response Team (CCRT) • Implementation of the CCRT has provided an effective • mechanism for timely communication of patient information, • and collaborative knowledge transfer among hospital staff • resulting in improved patient care and follow-up • The Situation Background Assessment Recommendation • (SBAR) communication tool is utilized by the CCRT for • clinical documentation
Post - CCRT Implementation Post CCRT Referral Survey The CCRT is an important service to have available…. Patient Safety Staff Safety
In addition, ongoing positive feedback from clinicians reflects an enhanced patient safety culture Improved mutual collaborative teamwork and knowledge transfer, and opportunities for improvement with lessons learned and debriefing Improved communication of patient issues, goals and plan of care Increased confidence and improved assessment skills and early identification and communication of problems Increased learning opportunities, clinical support, and continuous quality improvement Increased collaborative sharing and relationship building within our organization and with our LHIN and provincial colleagues Other Outcomes…
Post - CCRT Implementation Post CCRT Referral Survey • ….I have called the team to two of my patients and the presence of the team was greatly appreciated and furthermore the style and approach of the team was professional, reassuring, and respectful. (Dr. David Higgins, Chief of Staff) • ….One of the best additions at this hospital, a great advantage to decrease and diffuse critical situations. (anonymous) • ….Working with the CCRT did take time away from my other patients, but being part of the situation is a vital learning tool for future “situations”. (anonymous) • ….CCRT is the best thing the hospital has ever done. (anonymous)
CCRT CCRT