Download
1 / 1
10 likes | 202 Views
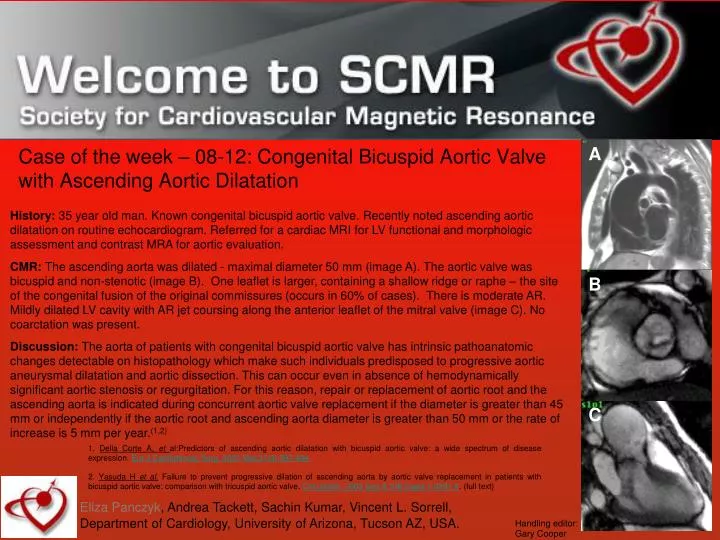
A. Case of the week – 08-12: Congenital Bicuspid Aortic Valve with Ascending Aortic Dilatation.

E N D
A Case of the week – 08-12: Congenital Bicuspid Aortic Valve with Ascending Aortic Dilatation History: 35 year old man. Known congenital bicuspid aortic valve. Recently noted ascending aortic dilatation on routine echocardiogram. Referred for a cardiac MRI for LV functional and morphologic assessment and contrast MRA for aortic evaluation. CMR: The ascending aorta was dilated - maximal diameter 50 mm (image A). The aorticvalve was bicuspid and non-stenotic (image B). One leaflet is larger, containing a shallow ridge or raphe – the site of the congenital fusion of the original commissures (occurs in 60% of cases). There is moderate AR. Mildly dilated LV cavity with AR jet coursing along the anterior leaflet of the mitral valve (image C). No coarctation was present. Discussion: The aorta of patients with congenital bicuspid aortic valve has intrinsic pathoanatomic changes detectable on histopathology which make such individuals predisposed to progressive aortic aneurysmal dilatation and aortic dissection. This can occur even in absence of hemodynamically significant aortic stenosis or regurgitation. For this reason, repair or replacement of aortic root and the ascending aorta is indicated during concurrent aortic valve replacement if the diameter is greater than 45 mm or independently if the aortic root and ascending aorta diameter is greater than 50 mm or the rate of increase is 5 mm per year.(1,2) B C 1. Della Corte A, et al:Predictors of ascending aortic dilatation with bicuspid aortic valve: a wide spectrum of disease expression. Eur J Cardiothorac Surg. 2007 Mar;31(3):397-404. 2. Yasuda H et al. Failure to prevent progressive dilation of ascending aorta by aortic valve replacement in patients with bicuspid aortic valve: comparison with tricuspid aortic valve. Circulation. 2003 Sep 9;108 Suppl 1:II291-4. (full text) Eliza Panczyk, Andrea Tackett, Sachin Kumar, Vincent L. Sorrell, Department of Cardiology, University of Arizona, Tucson AZ, USA. Handling editor: Gary Cooper