Download
1 / 57
921 likes | 5.62k Views
LEPROSY. Leprosy I Introduction Epidemiology Bacteriology Classification Clinical features. Leprosy II Reactions Diagnosis Treatment Rehabilitation. Introduction. Chronic granulomatous disease Caused by Mycobacterium leprae Mainly involves the peripheral nerves and skin

E N D
Leprosy I Introduction Epidemiology Bacteriology Classification Clinical features Leprosy II Reactions Diagnosis Treatment Rehabilitation
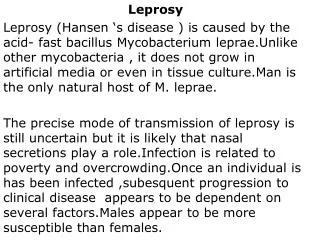
Introduction • Chronic granulomatous disease • Caused by Mycobacterium leprae • Mainly involves the peripheral nerves and skin • Other organs may involve: Mucosa of mouth Upper respiratory tract Eyes Bones Testes etc
Historical aspect of leprosy • Oldest disease known to mankind • Word leper comes from Greek word “scaling” • Earliest description from India in 600BC • Kustha Roga & attributed punishment or curse of God • M. leprae discovered in 1873 by Armauer Hansen • Referred as Hansen’s disease
Distribution • Prevalence • Wide distribution world-wide • Out of 122 countries, only 2 countries still have to reach the elimination goal Brazil and East Timor
Leprosy status in districtsMarch 2010 59 Districts with Prevalence rate less than 1 per 10,000 16 Districts with PR more than 1 per 10,000
Lepra bacilli • Obligate intracellular Gram positive and acid fast bacilli • Short, thick, pink stained rods • Size: 5 X 0.5 • Arrangement: Single or in cigar-shaped bundles or in “globi” • Affinity for Schwan cells & cells of R-E system • Cannot grow in vitro but can grow in • mice and • nine banded armadillos
Reservoir of infection • Main reservoir: Human being • Lepromatous case> Non lepromatous cases • Animal reservoirs • 9-banded armadillos • Chimpanzees • Mangabey monkeys
Portal of exit • Major portal of exit: Nose • LL cases harbour millions of M. leprae in their nasal mucosa • Ulcerated or broken skin of bacteriologically positive cases
Mode of transmission • Transmission by inhalation • Droplet infection • Transmission by contact • Skin to skin contact with infectious cases • Skin contact with soil & fomites
Incubation period • Long incubation period • Ranged: 6 months-40 years or more • Average: 2-5 years
Environmental factors • Humidity favors survival of M. leprae in environment • M. leprae remain viable in • Dried nasal secretions for 9 days • Moist soil at room temperature for 46 days • Overcrowding & lack of ventilation within households
Social factors • Often called a “social disease” • Social factors: • Poverty • Poverty related circumstances • Overcrowding • Poor housing • Lack of personal hygiene
IMPORTANCE OF CLASSIFICATION Identify the infectious cases – Epidemiological importance - Principal targets for treatment Identify the patients likely to develop the deformities and determine the prognosis Frame the line of treatment Helpful in planning and evaluation of leprosy control activities
Ridley-Jopling 1966 (Research purposes) Most widely accepted Based on clinical, bacteriological, immunological and histopathological parameters, which divide the leprosy into five recognizable groups Exhibits a spectral disease with varied clinical characteristics due to varied host immune response to bacilli
RIDLEY-JOPLING Tuberculoid (TT) Borderline Tuberculoid (BT) Borderline Borderline (BB) Borderline Lepromatous (BL) Lepromatous (LL)
Immunity in leprosy LL - multibacillary state with multiple lesions due to low immune response (+) TT -paucibacillary state, few lesions due to high immune response (-) BLHD LLHD BBHD BTHD TTHD
Contd.. Borderline forms (BB, BT and BL) lie between these two poles and are immunologically unstable, tending to move towards one of the polar forms
Immunology & bacteriology in leprosy (spectrum) (+++) (+++) Bacilli Immunity (++) (++) Bacilli Immunity (+) (+) (-) (-) LLHD BLHD BBHD BTHD TTHD
W H O classification(For chemotherapy – M. leprae) Paucibacillary Multibacillary Mid borderline – BB Borderline Lepromatous – BL Lepromatous – LL All smear positive cases Indeterminate - I Tuberculoid – TT Borderline Tuberculoid – BT If any of these have positive bacterial index they should be classified as multibacillary for multidrug therapy
Indeterminate Leprosy • Earliest & transitory stage • Hypopigmented macule with indistinct margins
Indeterminate Leprosy If untreated may progress towards tuberculoid, borderline or lepromatous leprosy Spontaneous regression may occur Usually negative for skin smear for AFB
TUBERCULOID LEPROSY Single or a few lesions Asymmetrically distributed on trunk and limbs Sharply defined, dry, erythematous or hypopigmented, anesthetic macules or plaques One or two nerves may be enlarged near the skin lesion SS for AFB: Negative Lepromin test may be strongly positive
Borderline Tuberculoid Single or multiple, asymmetrically distributed Macules or plaques of variable sizes with well-defined margins & satellite lesions Peripheral nerves enlarged asymmetrically Sensation: hyposthesia SS for AFB: may be seen Lepromin test may be weakly positive
Borderline Borderline Multiple erythematous macules & plaques Various sizes and shapes with punched out centre and ill defined slopping outer margin Tend to be symmetrical Nerves may be asymmetrically enlarged Sensation:+/- SS for AFB: seen +/- Lepromin test-usually negative, may be doubtful
Borderline Lepromatous Numerous, symmetrically distributed lesions Hypopigmented or erythematous irregularly shaped maculopapules, infiltrative nodules, or plaques, with smooth surfaces & ill defined borders, sloping outwards Nerves may be symmetrically or asymmetrically enlarged Sensation:+/- SS for AFB: numerous seen Lepromin test -negative
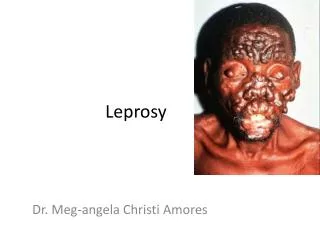
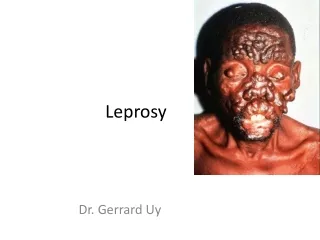
Lepromatous Leprosy Numerous macules, plaques, nodules or diffusely infiltrated lesions, symmetrically distributed on face, trunk and extremities with ill-defined margin which may be slightly hypopigmented or erythematous Symmetrical nerve enlargement is seen Sensation: normal SS for AFB: numerous seen Lepromin test - negative
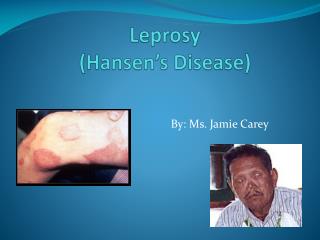
diffuse thickening of the skin, with loss of hair (eyebrows and eyelashes). saddle nose deformity leonine facies
General Findings • Eye The anterior chamber can be invaded in LL with resultant glaucoma and cataract formation. Iritis/Iridocyclitis • Testes May be involved in LL with resultant hypogonadism. • Systemic involvement – Respiratory, Bones, Kidneys, Lymph glands, etc.
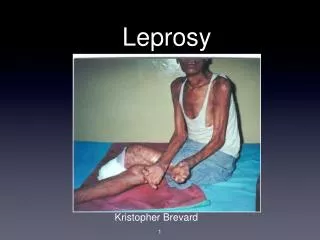
Nerve Involvement • Neural involvement leads to muscle weakness, muscle atrophy, severe neuritic pain, and contractures of the hands and feet. • Ulnar nerve commonly involved • Examination for sensations of hot and cold , pain and fine touch
Face Facial Nerve Lagophthalmos Facial droop Trigeminal Nerve Corneal anaesthesia