Download
1 / 50
500 likes | 771 Views
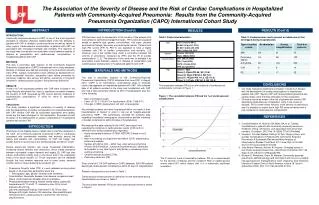
TM. Prepared for your next patient. Current Diagnosis & Treatment of Community-Acquired Pneumonia in Children Highlights of the PIDS/IDSA National Guidelines Samir S. Shah, MD, MSCE, FAAP Professor, Department of Pediatrics University of Cincinnati College of Medicine

E N D
TM Prepared for your next patient. Current Diagnosis & Treatment of Community-Acquired Pneumonia in Children Highlights of the PIDS/IDSA National Guidelines Samir S. Shah, MD, MSCE, FAAP Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Cincinnati Children's Hospital Medical Center
Disclaimers • Statements and opinions expressed are those of the authors and not necessarily those of the American Academy of Pediatrics. • Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter has complete and independent control over the planning and content of the presentation, and is not receiving any compensation from Mead Johnson for this presentation. The presenter’s comments and opinions are not necessarily those of Mead Johnson. In the event that the presentation contains statements about uses of drugs that are not within the drugs' approved indications, Mead Johnson does not promote the use of any drug for indications outside the FDA-approved product label.
Disclaimers continued • I have no financial conflicts of interest to disclose. • I have not received any compensation for preparing and presenting this webinar. • I served as Associate Chair of the Pediatric Infectious Diseases Society/Infectious Diseases Society of America Pneumonia Guidelines Committee, the topic of this presentation. • Sources of current research support: • National Institute of Allergy and Infectious Diseases • Agency for Healthcare Research and Quality • Children’s Hospitals Association • Robert Wood Johnson Foundation
Objectives • Discuss the rationale for creating pediatric community-acquired pneumonia (CAP) national guidelines. • Describe currently recommended diagnostic and treatment strategies for CAP in the United States.
Why Do We Need Guidelines? • Role of guidelines • Assist in healthcare decision-making • Reduce variation in clinical practice • Lead to better patient care and outcomes • Only as good as the evidence on which they are based • Most useful for conditions with substantial variation in clinical practice and outcomes
Context for the US Guidelines KronmanMP. Pediatrics. 2011; Shah SS. J HospMed. 2011; Lee GE. Pediatrics. 2010; Shah SS. PediatrPulmonol. 2010 • CAP is the most common serious childhood infection in the US. • 3 million outpatient visits each year • >150,000 hospitalizations each year • Up to 15% of children hospitalized with CAP have a serious pneumonia-associated complication such as empyema. • In the US, there is substantial variation across hospitals and physicians in diagnosis, treatment, and outcomes.
Diagnostic Testing for CAP at 43 US Hospitals Brogan TV. Pediatr Infect Dis J. 2012
Treatment for CAP at 43 US Hospitals Data from Ambroggio LV, et al. Pediatr Infect Dis J. 2012
Available Free Online and In Print • Guidelines available at: www.idsociety.org • Bradley JS, Byington CL, Shah SS, and Alverson B, Carter ER, Harrison C, Kaplan SL, Mace S, McCracken G, Moore M, St. Peter S, Stockwell J, Swanson JT. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:e25–e76 • Bradley JS, Byington CL, Shah SS, and Alverson B, Carter ER, Harrison C, Kaplan SL, Mace S, McCracken G, Moore M, St. Peter S, Stockwell J, Swanson JT. Executive Summary: The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:617–630
Consensus Development Based on Evidence • 92 recommendations • Consensus development based on evidence • GRADE working group (Grading of Recommendations, Assessment, Development, and Evaluation) • Method of assigning strength of recommendation and quality of evidence to each recommendation Strength of Recommendation (Strong or Weak) Quality of Evidence (High, Moderate, or Low)
Evidence-Based Guidelines • Clinical Recommendations • Site of care • Diagnostic testing • Anti-infective treatment • Adjunctive treatment • Management of the child not responding to treatment • Discharge criteria • Prevention • Future research
Evidence-Based Guidelines • Clinical Recommendations • Site of care • Diagnostic testing • Anti-infective treatment • Adjunctive treatment • Management of the child not responding to treatment • Discharge criteria • Prevention • Future research
Outline • Diagnostic Testing • Pulse oximetry • Chest x-ray • Blood culture • Atypical bacteria testing • Viral testing • Complete blood counts • Anti-Infective Treatment
Definition of CAP • CAP is the presence of signs and symptoms of pneumonia in a previously healthy child due to an infection acquired outside of the hospital. • Guideline scope • Age 3 months – 18 years • Exclusionary conditions • Immune deficiency • Chronic lung disease (e.g., cystic fibrosis) • Mechanical ventilation
Initial Chest X-Ray—Rationale Swingler GH. Cochrane Database Syst Rev. 2008; Swingler GH. Lancet. 1998; Novack V. J Intern Med. 2006; Alario AJ. J Pediatr. 1987; Grossman LK. Ann Emerg Med. 1988 • Chest x-rays (CXRs) not routinely required for outpatient CAP • CXRs: • Do not reliably distinguish bacterial from viral CAP or among the various bacterial pathogens • Impractical in office setting • Often requires travel to a separate facility • Barriers to physicians obtaining timely results • CXR in outpatient setting infrequently changes clinical management • Guideline provides guidance on when to perform CXR in outpatient setting
Repeat Chest X-Ray—Rationale Gibson NA. BMJ. 1993; Virkki R. PediatrPulmonol. 2005; Grossman LK. Pediatrics. 1979; Wacogne I. Arch Dis Child. 2003; Heaton P. N Z Med J. 1998; Bruns AH. Clin Infect Dis. 2007 • Repeat CXRs commonly identify persistent or residual abnormalities 3–6 weeks later. • Abnormalities rarely alter management. • Abnormalities do not predict treatment failure or worse clinical outcome. • Repeat CXRs represent unnecessary radiation exposure to infants and children.
Blood Cultures—Rationale Bonadio WA. PediatrEmergCare. 1988; Hickey RW. Ann EmergMed. 1996; Shah SS. Arch PediatrAdolescMed. 2003; Shah SS. Pediatr Infect Dis J. 2011 • Outpatient • Infrequently identifies pathogens (<2%) • False-positives more common than true positives at some hospitals • Rarely informs outpatient management
Blood Cultures—Rationale Bonadio WA. PediatrEmergCare. 1988; Hickey RW. Ann EmergMed. 1996; Shah SS. Arch PediatrAdolescMed. 2003; Shah SS. Pediatr Infect Dis J. 2011 • Outpatient • Infrequently identifies pathogens (<2%) • False-positives more common than true positives at some hospitals • Rarely informs outpatient management • Inpatient • Positive in ~3% of uncomplicated pneumonia • Positive in ~15% with empyema • Allows for culture-directed therapy when positive • Provides local epidemiologic data
Atypical Bacteria Testing―Rationale Heiskanen-Kosma T. Pediatr Infect Dis J. 1998; Michelow IC. Pediatrics. 2004; Korppi M. Respirology. 2004; Thurman KA. Clin Infect Dis. 2009 • Evolving understanding of M. pneumoniae epidemiology • Increasingly identified in younger children • Rapid tests (IgM and PCR) available • Variable test accuracy • Treatment is not mandatory, especially with low likelihood of infection (e.g., negative test), as benefit of macrolide antibiotics uncertain
Diagnostic Testing—Viral Pathogens • Antibacterial therapy is not necessary in children, either outpatients or inpatients, with a positive test for influenza virus in the absence of clinical, laboratory, or radiographic findings that suggest bacterial co-infection. Strong recommendation; High-quality evidence
Viral Testing—Rationale Bonner AB. Pediatrics. 2003; Esposito S. Arch Dis Child. 2003; Iyer SB. AcadEmerg Med. 2006; Benito-Fernandez J. Pediatr Infect Dis J. 2006 • Influenza testing • Positive tests reduce antibiotic use and ancillary testing (e.g., CXR, CBC) by >50%. • Positive tests guide antiviral treatment decisions. • Early treatment improves outcomes.
Complete Blood Count—Rationale Waters AM. J Pediatr. 2007; Banerjee R. Pediatr Infect Dis J. 2011; Korppi M. EurRespir J. 1997 • Anemia and thrombocytopenia may suggest hemolytic-uremic syndrome. • Rarely an occult process. • WBC count has poor specificity for diagnosis of bacterial pneumonia. • WBC elevated in many children with CAP. • Most children with elevated WBC do nothave CAP. • WBC does not reliably distinguish bacterial from viral CAP.
Antibiotic Choice—Rationale KyawMH. N Engl J Med. 2006 • S. pneumoniae remains most common bacterial cause of CAP • Decreasing S. pneumoniae antibiotic resistance • >50% decrease in penicillin-non-susceptible infections • >50% decrease strains in resistance to multiple antibiotics
Antibiotic Choice—Rationale Yu VL. Clin Infect Dis. 2003; Perez-TralleroE. J AntimicrobChemother. 1998; Perez-TralleroE. J Chemother. 2001 • Penicillin resistance is notassociated with treatment failure for non-CNS S. pneumoniae infections. • In vitro, bactericidal activity achieved at low concentrations relative to MIC • In vivo, high and sustained concentrations achieved in serum and lung • Amoxicillin administered at 80 mg/kg/day • Ampicillin administered at 300 mg/kg/day
Antibiotic Choice—Rationale Yu VL. Clin Infect Dis. 2003; Perez-TralleroE. J AntimicrobChemother. 1998; Chung J. Anaesth Intensive Care. 2011 • Macrolide resistance and 2nd generation cephalosporin resistance are associated with treatment failure for non-CNS S. pneumoniae infections. • Vancomycin • Not necessary for S. pneumoniae • MRSA less common and rarely “occult” • Challenges • Poor lung penetration compared with aminopenicillins • Associated with nephrotoxicity • May require monitoring trough concentrations or continuous infusion
Minimizing Resistance―Duration of Therapy Treatment for the shortest effective duration will minimize exposure of both pathogens and normal microbiota, and minimize the selection for resistance. Strong recommendation;Low-quality evidence Treatment courses of 10 days have been best studied. Shorter courses may be just as effective, particularly for more mild disease managed on an outpatient basis. Strong recommendation;Moderate-quality evidence Infections caused by certain pathogens, notably CA-MRSA, may require longer treatment than those caused by S. pneumoniae. Strong recommendation;Moderate-quality evidence
Final Thoughts Guidelines are only as good as the evidence on which they are based.
Final Thoughts Developing guidelines is relatively easy compared to implementing them.
For more information… On this topic and a host of other topics, visit www.pediatriccareonline.org. Pediatric Care Online is a convenient electronic resource for immediate expert help with virtually every pediatric clinical information need. Must-have resources are included in a comprehensive reference library and time-saving clinical tools. Haven't activated your Pediatric Care Online trial subscription yet?It's quick and easy: simply follow the steps on the back of the card you received from your Mead Johnson representative. Haven't received your free trial card?Contact your Mead Johnson representative or call 888/363-2362 today.