Download
1 / 42
480 likes | 1.11k Views
Workshop 12 Group 3 Section D. Mitral Valve Prolapse. MM 23 y/o . Chief complaint : Palpitations History of Present Illness:. Review of Systems. No dizziness, nor loss of consciousness No cough or colds No PND or orthopnea. Physical Examination. Conscious, coherent, ambulatory

E N D
Workshop 12 Group 3 Section D Mitral Valve Prolapse
MM 23 y/o Chief complaint : Palpitations History of Present Illness:
Review of Systems • No dizziness, nor loss of consciousness • No cough or colds • No PND or orthopnea
Physical Examination • Conscious, coherent, ambulatory • BP 110/70 CR 80/min regular RR 16/min BMI 19 • Symmetrical chest expansion, narrow AP diameter of the chest, no retractions, clear breath sounds • Adynamicprecordium, AB at 5th LICS MCL no murmurs, (+) midsystolic click follwed by 2/6 mid-systolic crescendo murmur noted at the apex
Laboratory and Ancillary Tests • 2D Echo-doppler: • Mitral Valve Prolapse, Anterior Mitral Valve Leaflet with moderate MR • Slightly dilated left atrium woth no evidence of thrombus • 12 Lead ECG • Sinus rhythm • Occasional premature atrial complexes
1. What are the common physical examination findings of MVP?
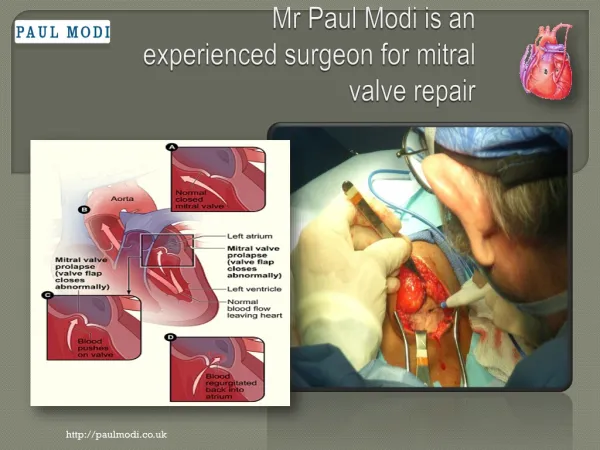
Common PE findings of MVP • Auscultation • Mid – late (non- ejection) systolic click (0.14s) after S1 • Systolic clicks: multiple and may be follwed by a high-pitched, late systolic crescendo-decrescendo murmur, “ whooping” or “honking”- heard best at apex • Early click-murmur • Standing, during valsalva maneuver, and with ant intervention that decreases LV volume • Delayed and complex click-murmur • Squatting, isometric exercises which increase LV volume
Population group • 14 - 30 years old • Women • Increased familial incidence Reference: Fauci et al. Harrison’s Principles of Internal Medicine, 17th ed.
Common Symptoms * Patients are mostly asymptomatic Others may manifest with: • Easy fatigability • Shortness of breath • Palpitation • Non-anginal chest pain • Light-headedness • Syncope Reference: Fauci et al. Harrison’s Principles of Internal Medicine, 17th ed.
Uncommon Symptoms • Transient ischemic attacks • Congestive cardiac failure • Endocarditis • in MR associated with MVP • Sudden death Reference: Fauci et al. Harrison’s Principles of Internal Medicine, 17th ed.
Symptoms related to autonomic dysfunction are usually associated with genetic inheritance: • Anxiety • Panic attacks • Arrhythmias • Exercise intolerance • Palpitations • Atypical chest pain • Fatigue • Orthostasis • Syncope or presyncope • Neuropsychiatric symptoms Thakkar, B. (2008) Mitral Valve Prolapse < http://emedicine.medscape.com/article>
Symptoms related to progression of mitral regurgitation : • Fatigue • Dyspnea • Exercise intolerance • Orthopnea • Paroxysmal nocturnal dyspnea (PND) • Progressive signs of congestive heart failure (CHF) Thakkar, B. (2008) Mitral Valve Prolapse < http://emedicine.medscape.com/article>
In most studies, MVP has a complication rate of less than 2 percent per year2,15 . • The age-adjusted survival rate in men and women with MVP is similar to that in patients without this common clinical disorder
Complications of Mitral Valve Prolapse Atrial fibrillation and other arrhythmias Congestive heart failure Pulmonary hypertension Ruptured mitral valve chordae Infective endocarditis Central nervous system embolic events O'Rourke RA. The mitral valve prolapse syndrome. In: Chizner MA, ed. Classic teachings in clinical cardiology. Cedar Grove, N.J.: Laennec, 1996:1049-70.
Congestive Heart Failure Gradual progression of mitral regurgitation progressive dilation of the left atrium and left ventricle atrial fibrillation, moderate to severe mitral regurgitation LV dysfunction congestive heart failure
Infective Endocarditis • A serious complication of MVP • MVP is the leading predisposing cardiovascular disorder in patients with endocarditis. • Because the absolute incidence of endocarditis is extremely low in the entire MVP population, the risk of its developing in these patients has been a subject of considerable debate.
Thromboembolic Events • Rarely, fibrin emboli may cause visual problems related to occlusion of the ophthalmic or posterior cerebral circulation. • Patients younger than 45 years who have MVP are at greater risk for cerebrovascular accidents than would be expected in similar patients without MVP. • Therefore, it has been recommended that antiplatelet drugs such as aspirin or anticoagulants be administered to patients with MVP who have a history of suspected cerebral emboli
4. What population group is associated with an increased predilection for MVP?
Idiopathic MVP Cause of MVP may be a genetically determined collagen disorder Electron microscopy: fragmentation of collagen fibrils Reduction in the production of type III collagen Fauci, et al. 2008. Harrison’s Principles of Internal Medicine, 17th ed. Venugopalan. 2008. Mitral Valve Prolapse. <http://emedicine.medscape.com/article/890425-overview>
Hereditary Connective Tissue Disorders • Mitral valve prolapse is a frequent finding in patients of this population • Others: Fragile X syndrome, Martin-Bell syndrome, Polycystic kidney disease (adult type), Periarteritisnodosa Fauci, et al. 2008. Harrison’s Principles of Internal Medicine, 17th ed. Venugopalan. 2008. Mitral Valve Prolapse. <http://emedicine.medscape.com/article/890425-overview>
Clinical approach to determination of the need for prophylaxis in patients with suspected MVP Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
A reasonable approach for endocarditis prophylaxis should consider the following: • the degree to which the patient’s underlying condition creates a risk of endocarditis • the apparent risk of bacteremia with the procedure • the potential adverse reactions of the prophylactic antimicrobial agent to be used; and the cost-benefit aspects of the recommended prophylactic regimen Failure to consider all of these factors may lead to overuse of antimicrobial agents, excessivecost, and risk of adverse drug reactions Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Prophylaxis is recommended in individuals who have a higher risk for developing endocarditis than the general population and is particularly important for individuals in whom endocardial infection is associated with high morbidity and mortality Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Endocarditis prophylaxis recommended High-risk category • Prosthetic cardiac valves • Previous bacterial endocarditis • Complex cyanotic congenital heart disease Eg. Single ventricle states, Transposition of the great arteries, Tetralogyof Fallot • Surgically constructed systemic pulmonary shunts or conduits Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Moderate-risk category • Acquired valvular dysfunction (eg, rheumatic heart disease) • Hypertrophic cardiomyopathy • Mitral valve prolapse with valvular regurgitation and/or thickened leaflets Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Endocarditis prophylaxis NOT recommended Negligible-risk category • Isolated secundumatrialseptal defect • Surgical repair of ASD, VSD or PDA • Previous coronary artery bypass graft surgery • Mitral valve prolapse without valvular regurgitation • Physiologic, functional, or innocent heart murmurs • Previous Kawasaki disease without valvular dysfunction • Previous rheumatic fever without valvular dysfunction • Cardiac pacemakers and implanted defibrillators Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Prophylaxis • Prophylaxis at the time of cardiac surgery should be directed primarily against staphylococci and should be of short duration • First-generation cephalosporins are most often used • Prophylaxis is most effective when given perioperatively in doses that are sufficient to assure adequate antibiotic concentrations during and after the procedure • Antibiotics should be used only during the perioperative period - initiated shortly before a procedure and should not be continued no more than 6 to 8 hours • In the case of delayed healing, or of a procedure that involves infected tissue, it may be necessary to provide additional doses of antibiotics
Prophylaxis • Antimicrobial prophylaxis administered within 2 hours following the procedure will provide effective prophylaxis Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Streptococcus viridansis the most common cause of endocarditis following: • dental or oral procedures • certain upper respiratory tract procedures • bronchoscopy with a rigid bronchoscope • surgical procedures that involve the respiratory mucosa • esophageal procedures
Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
The recommended standard prophylactic regimen for all these procedures is a single dose of oral amoxicillin to be administered 1 hour before the anticipated procedure • Adult dose is 2.0 g • Pediatric dose is 50 mg/kg (not to exceed adult dose) • For individuals who are unable to take or unable to absorb oral medications, parenteralAmpicillin sodium is recommended Durack DT. Prevention of infective endocarditis. N Engl J Med. 1995
Individuals who are allergic to penicillin • Clindamycinhydrochloride • Azithromycin or clarithromycin • When parenteral administration is needed in an individual who is allergic to penicillin, clindamycin phosphate is recommended Durack DT. Prevention of infective endocarditis. N Engl J Med. 1995
Prophylaxis • Enterococcusfaecalisis the most common cause of bacterial endocarditis that occurs following genitourinary and gastrointestinal tract surgery or instrumentation • Antibiotic prophylaxis should be directed primarily against Enterococci
Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association
High-risk patients • Ampicillin plus gentamicin • High-risk patients allergic to ampicillin/amoxicillin • Vancomycin plus gentamicin • Moderate-risk patients • Amoxicillin or ampicillin • Moderate-risk patients allergic to ampicillin/amoxicillin • Vancomycin Prevention of Bacterial Endocarditis: Recommendations by the American Heart Association