Download
1 / 1
20 likes | 336 Views
B12 DEFICIENCY PRESENTING AS PANCYTOPENIA IN PREGNANCY: A CASE REPORT AND REVIEW OF LITERATURE Nazimah Idris 1 Akmal Hisyam Arshad 2 1 International Medical University Malaysia 2 Ministry of Health Malaysia. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. CONCLUSIONS. INTRODUCTION.

E N D
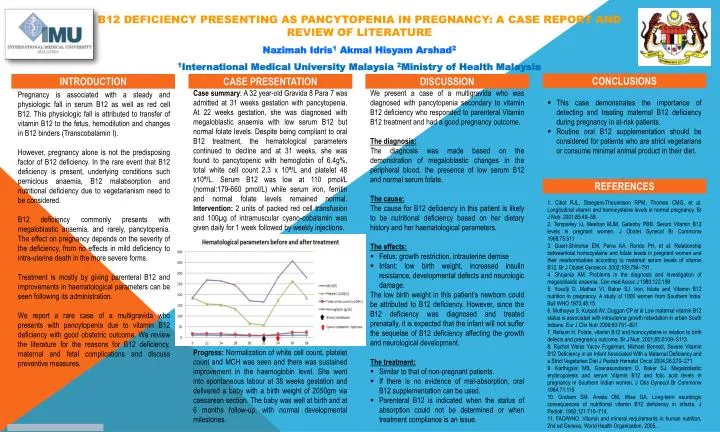
B12 DEFICIENCY PRESENTING AS PANCYTOPENIA IN PREGNANCY: A CASE REPORT AND REVIEW OF LITERATURE Nazimah Idris1 Akmal Hisyam Arshad2 1International Medical University Malaysia 2Ministry of Health Malaysia OPTIONALLOGO HERE OPTIONALLOGO HERE CONCLUSIONS INTRODUCTION CASE PRESENTATION DISCUSSION Case summary: A 32 year-old Gravida 8 Para 7 was admitted at 31 weeks gestation with pancytopenia. At 22 weeks gestation, she was diagnosed with megaloblastic anaemia with low serum B12 but normal folate levels. Despite being compliant to oral B12 treatment, the hematological parameters continued to decline and at 31 weeks, she was found to pancytopenic with hemoglobin of 6.4g%, total white cell count 2.3 x 10⁹/L and platelet 48 x10⁹/L. Serum B12 was low at 110 pmol/L (normal:179-660 pmol/L) while serum iron, ferritin and normal folate levels remained normal. Intervention: 2 units of packed red cell transfusion and 100µg of intramuscular cyano-cobalamin was given daily for 1 week followed by weekly injections. Progress: Normalization of white cell count, platelet count and MCH was seen and there was sustained improvement in the haemoglobin level. She went into spontaneous labour at 38 weeks gestation and delivered a baby with a birth weight of 2050gm via caesarean section. The baby was well at birth and at 6 months follow-up, with normal developmental milestones. • We present a case of a multigravida who was diagnosed with pancytopenia secondary to vitamin B12 deficiency who responded to parenteral Vitamin B12 treatment and had a good pregnancy outcome. • The diagnosis: • The diagnosis was made based on the demonstration of megaloblastic changes in the peripheral blood, the presence of low serum B12 and normal serum folate. • The cause: • The cause for B12 deficiency in this patient is likely to be nutritional deficiency based on her dietary history and her haematological parameters. • The effects: • Fetus: growth restriction, intrauterine demise • Infant: low birth weight, increased insulin resistance, developmental defects and neurologic damage. • The low birth weight in this patient’s newborn could be attributed to B12 deficiency. However, since the B12 deficiency was diagnosed and treated prenatally, it is expected that the infant will not suffer the sequelae of B12 deficiency affecting the growth and neurological development. • The treatment: • Similar to that of non-pregnant patients. • If there is no evidence of mal-absorption, oral B12 supplementation can be used. • Parenteral B12 is indicated when the status of absorption could not be determined or when treatment compliance is an issue. • This case demonstrates the importance of detecting and treating maternal B12 deficiency during pregnancy in at-risk patients. • Routine oral B12 supplementation should be considered for patients who are strict vegetarians or consume minimal animal product in their diet. Pregnancy is associated with a steady and physiologic fall in serum B12 as well as red cell B12. This physiologic fall is attributed to transfer of vitamin B12 to the fetus, hemodilution and changes in B12 binders (Transcobalamin I). However, pregnancy alone is not the predisposing factor of B12 deficiency. In the rare event that B12 deficiency is present, underlying conditions such pernicious anaemia, B12 malabsorption and nutritional deficiency due to vegetarianism need to be considered. B12 deficiency commonly presents with megaloblastic anaemia, and rarely, pancytopenia. The effect on pregnancy depends on the severity of the deficiency, from no effects in mild deficiency to intra-uterine death in the more severe forms. Treatment is mostly by giving parenteral B12 and improvements in haematological parameters can be seen following its administration. We report a rare case of a multigravida who presents with pancytopenia due to vitamin B12 deficiency with good obstetric outcome. We review the literature for the reasons for B12 deficiency, maternal and fetal complications and discuss preventive measures. REFERENCES 1. Cikot RJL, Steegers-Theunissen RPM, Thomas CMG, et al. Longitudinal vitamin and homocysteine levels in normal pregnancy. Br J Nutr. 2001;85:49–58. 2. Temperley IJ, Meehan MJM, Gatenby PBB. Serum Vitamin B12 levels in pregnant women. J Obstet Gynecol Br Commonw 1968;75:511 3. Guerr-Shinohar EM, Paiva AA, Rondo PH, et al. Relationship betweentotal homocysteine and folate levels in pregnant women and their newbornbabies according to maternal serum levels of vitamin B12. Br J Obstet Gynaecol. 2002;109:784–791. 4. Shojania AM. Problems in the diagnosis and investigation of megaloblastic anaemia. Can med Assoc J 1980;122:199 5. Yusufji D, Mathan VI, Baker SJ. Iron, folate and Vitamin B12 nutrition in pregnancy. A study of 1000 women from Southern India. Bull WHO 1973;48:15. 6. Muthayya S, Kurpad AV, Duggan CP et al Low maternal vitamin B12 status is associated with intrauterine growth retardation in urban South Indians. Eur J Clin Nutr 2006;60:791–801 7. Refsum H. Folate, vitamin B12 and homocysteine in relation to birth defects and pregnancy outcome. Br J Nutr. 2001;85:S109–S113. 8. Rachel Weiss Yacov Fogelman, Michael Bennett, Severe Vitamin B12 Deficiency in an Infant Associated With a Maternal Deficiency and a Strict Vegetarian Diet J Pediatr Hematol Oncol 2004;26:270–271 9. Karthigaini MB, Gnanasundaram D, Baker SJ. Megaloblastic erythropoiesis and serum Vitamin B12 and folic acid levels in pregnancy in Southern Indian women. J Obs Gynecol Br Commonw 1964;71:115 10. Graham SM, Arvela OM, Wise GA. Long-term neurologic consequences of nutritional vitamin B12 deficiency in infants. J Pediatr. 1992;121:710–714. 11. FAO/WHO. Vitamin and mineral requirements in human nutrition, 2nd ed.Geneva, World Health Organization, 2005..