Download
1 / 35
420 likes | 3.78k Views
Vulvar Cancer. Kathleen M. Schmeler, M.D. Assistant Professor Department of Gynecologic Oncology. Vulvar Cancer. 4th most common gynecologic cancer in USA (following uterus, ovary and cervix) Comprises 5% of gynecologic malignancies

E N D
Vulvar Cancer Kathleen M. Schmeler, M.D. Assistant Professor Department of Gynecologic Oncology
Vulvar Cancer 4th most common gynecologic cancer in USA (following uterus, ovary and cervix) Comprises 5% of gynecologic malignancies There are an estimated 3,500 new cases and 870 associated deaths per year in USA Mean age at diagnosis is 65y, but is decreasing
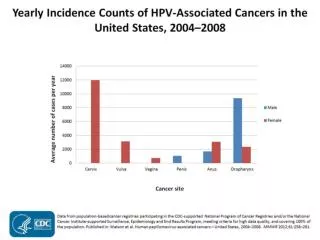
Vulvar Cancer Risk Factors: Cigarette smoking Human Papilloma Virus (HPV) infection Immunosuppression Chronic vulvar conditions such as lichen sclerosus VIN/CIN Prior history of cervical cancer
Vulvar Cancer Two pathways of vulvar carcinogenesis: HPV infection (60%) Chronic inflammatory (vulvar dystrophy) or autoimmune processes
Clinical Manifestations Most patients present with a single vulvar plaque, ulcer or mass Labia majora is the most common site Lesions are multifocal in 5% of cases so complete examination of the vulva, perianal area, vagina and cervix is required A synchronous second malignancy is found in 22% of cases, usually CIN/cervical cancer
Clinical Manifestations Pruritus is the most common presenting symptom (especially if associated with vulvar dystrophy such as lichen sclerosus) Vulvar bleeding or discharge Dysuria Enlarged groin lymph node
Diagnosis Biopsy of gross lesions If no gross lesion present but high clinical suspicion, perform colposcopy with 5% acetic acid solution
Types of Vulvar Cancer Squamous cell carcinoma (>90% of cases) Melanoma Sarcoma Basal cell carcinoma Verrucous carcinoma Adenocarcinoma (Bartholin gland) Breast carcinoma (ectopic breast tissue in milk line that extends to perineum)
Squamous Cell Carcinoma (SCCA) Most common type (>90%) Two subtypes: 1. Warty/Basaloid: associated with HPV infection younger women 2. Keratinizing/Simplex/Differentiated: associated with vulvar dystrophies (e.g. lichen sclerosus) NOT HPV related older women
Treatment of SCCA Vulva Historically all patients were treated with radical vulvectomy and en-bloc inguinal-femoral lymphadenectomy through one incision (“Butterfly” or “Longhorn” incision) Significant morbidity was associated with this approach, including wound breakdown, lymphedema and sexual dysfunction Alternative surgical procedures that remove less of the vulva and surrounding skin are now used (“three-incision technique”)
Treatment of SCCA Vulva Wide Radical Excision (WRE): Excision of vulvar lesion down to the fascia of the urogenital diaphragm 2 cm tumor-free margin
Treatment of SCCA Vulva Inguinal-Femoral Lymphadenectomy: Removal of the superficial inguinal and deep femoral lymph nodes Performed through separate incisions from the vulvar resection (“three-incision technique”) Unilateral lymphadenectomy may be performed if unifocal lesion that is lateral (>2 cm from midline) Sentinel lymph node biopsy is appropriate as an alternative to a complete inguinal-femoral lymphadenectomy in some cases
Treatment of SCCA Vulva Radiation Therapy: Indicated if positive margins after WRE if re-excision not possible or desirable (i.e. around the clitoris or anal sphincter) Indicated if positive inguinal/pelvic nodes Radiation in combination with chemotherapy is an alternative to surgery in women with stage III/IVA disease
Treatment of SCCA Vulva Chemotherapy: Indicated for metastatic disease (stage IVB) Similar regimens as those used for metastatic cervical cancer Platinum-based Treatment is palliative
Treatment of Recurrent Disease Local recurrence treated with surgical re-excision For large local recurrence, pelvic exenteration may be required Inguinal lymph node recurrences have a much worse prognosis - treated with surgery and/or radiation therapy Chemotherapy used for distant disease
Melanoma of the Vulva 2nd most common type of vulvar cancer (5-6%) Occurs more frequently in white women Mean age at diagnosis is 68y (in contrast, cutaneous melanomas of other sites usually develop before age 45y) Usually pigmented lesion but amelanotic lesions also occur Treatment is wide local excision with 2 cm margins and sentinel lymph node biopsy +/- treatment with chemotherapy and/or biologic agents
Basal Cell Carcinoma 2% of vulvar cancers Usually occur in white, postmenopausal women May be locally invasive but usually do not metastasize Slow-growing Treatment is wide local excision
Paget Disease of the Vulva <1% of vulvar malignancies Most patients are postmenopausal and Caucasian Similar in appearance to Paget disease of the breast Most common presenting symptom is pruritus Lesion is usually well demarcated with slightly raised edges and a red background, dotted with small pale islands Usually multifocal
Paget Disease of the Vulva Treatment is wide local excision There is a high rate of local recurrence, even with negative surgical margins Treatment for recurrence is re-excision 4-17% of women have an underlying invasive adenocarcinoma of the vulva 20-30% of women have a synchronous malignancy (breast, rectum, bladder, urethra, cervix or ovary)
Summary – Vulvar Cancer Comprises 5% of gynecologic malignancies 2 pathways of vulvar carcinogenesis: HPV infection (60%) Chronic inflammatory (vulvar dystrophy) Most common histology is squamous cell carcinoma Treatment includes surgery, radiation and/or chemotherapy depending on stage