Download
1 / 12
120 likes | 337 Views
Fusarium keratitis in a tertiary eye care centre in India. Sujata Das, MS, FRCS Savitri Sharma, MD Samir Mahapatra , MS Srikant K Sahu , MS. L V Prasad Eye Institute Bhubaneswar, India, 751024 sujatadas@lvpei.org.

E N D
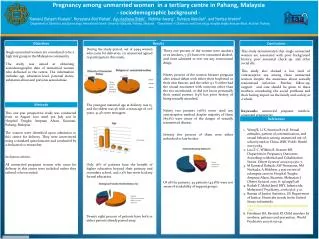
Fusariumkeratitis in a tertiary eye care centre in India Sujata Das, MS, FRCS Savitri Sharma, MD SamirMahapatra, MS Srikant K Sahu, MS L V Prasad Eye Institute Bhubaneswar, India, 751024 sujatadas@lvpei.org Authors do not have any financial or conflicting interests to disclose
Introduction • Fungal keratitis continues to be a cause of concern to ophthalmologists. • It accounts for 30 to 50% of all cases of microbial keratitis in developing countries.# • Increased awareness coupled with improved laboratory and in vivo diagnostic techniques have led to an increase in the frequency of correct diagnosis and consequent increase in prevalence of the disease.@ • Srinivasan M, et al. Br J Ophthalmol 1997; 81: 965-971. • Gopinathan U, et al. Cornea 2002; 21: 555-559. • Dunlop AA, et al. Aust N Z J Ophthalmol 1994; 22: 105-110. • Hagan M, et al. Br J Ophthalmol 1995; 79: 1024-1028. • O’Brien TP, Rhee P. In Textbook of Ocular Pharmacology. Hagerstown: Lipincott-Raven, 1997: 587-607. • O’Day D. In Ocular Infection and Immunity. St Louis: Mosbey, 1996: 1048-1061.
Introduction • The epidemiological features of fungal keratitis vary across geographic regions and climatic conditions. • Fungal keratitis occurs more frequently in warm, and dry climate than in temperate zones. • Fusarium and Aspergillus species are the most common fungi isolated from patients in tropical regions. • The purpose of the study was to report clinical and microbiological profile of Fusariumkeratitis.
Material and Methods • A retrospective analysis of medical records was done to study the clinical and microbiological profile of 42 consecutive culture-proven Fusariumkeratitis patients presented at the corneal unit of L V Prasad Eye Institute, Bhubaneswar, between November 2006 & July 2009. • The following data were collected from each record: age, sex, predisposing risk factor, clinical presentation, microbiological result, mode of management, and final outcome. • All patients had undergone detailed clinical evaluation and slit-lamp examination.
Material and Methods As a part of standard protocol, corneal scrapings were obtained from all microbial keratitis and subjected to the following : Placing on glass slide Smearing on glass slides Gram Giemsa KOH/CFW Thio BHI NNA( E. coli ) CA (CO2) SDA PDA BA (O2+) BA (O2-)
Results • Mean age of patients was 47±17 (range: 4-95, median: 45) years. • Eleven eyes (26.2%) had history of injury. • Mean duration of symptom was 17±14 (range: 3-60, median: 10) days. • Hypopyon was present in 15 (35.7%) cases. • Satellite lesion was not present in any eye. 42.86% 57.14%
Results • Thirty six (85.7%) cases were smear-positive for fungus. • In 3 cases microconidia was observed in direct smear examination. • Fusariumsolaniwas the most common (45.2%) fungi. • Five patients had associated bacterial infection. • All 3 cases where microconidia was present in direct smear examination were identified as Fusariumsolaniin culture. • The mean time to positive culture was 1.8±1 days.
Microbiological Examination Giemsa 1000 SDA BA CA
Adventitious Sporulation LCPB 400 CFW 200 Gram 1000 Gram 1000
Results • Twenty one (50%) patients underwent adjunctive surgical procedure • Tissue adhesive application : n = 9; • Therapeutic penetrating keratoplasty : n = 13; • Anterior chamber wash + Intracameral antifungal : n = 4; • Evisceration : n = 3. • 16.7% and 41.5% patients had visual acuity of <20/200 during presentation and final follow-up respectively. • Eighteen patients had improvement in visual acuity.
Conclusion • Fusariumkeratitis may present after trauma without any satellite lesion and needs surgical intervention in 50% cases. • Smears of corneal scrapings often disclosed hyphae, and culture media showed growth within 3 days. • Microconidia in smear examination may be suggestive of Fusariumsolani.