Download
1 / 25
250 likes | 265 Views
Explore the intricate world of single channel analysis and channelopathies, delving into topics like exponential decay, Hodgkin-Huxley kinetics, ion channel pathologies, and more. Understand how mutations in ion channel genes lead to diseases and syndromes. Discover the complexities of channelopathies and their impact on health.

E N D
Single Channel Analysis and Channelopathies Jim Huettner
Lecture Overview • Recording single channels • Transitions between states • Exponential decay • Analyzing channel recordings • Hodgkin-Huxley kinetics • Ball and chain inactivation • Ion channel and transporter pathologies
theory of analysis Radioactive Decay – Macroscopic Kinetics X → Y dX / dt = - X X(t) = X0 e - t = 1 /
analyzing single ion channels current time
mean open time = topen = 1 / a = 1 / closing rate constant b exponential distribution of lifetimes
two state model analysis Po = O/(O+C) = a/(a+b) [3] Ot = -(O¥ - Oo)e-t / t + O¥ [4] t = 1/(a+b) [5]
exponential relaxation Starting with all channels closed, the fraction of open channels increases exponentially with Tau = 1 / (a + b) and maximal open fraction = a/ (a + b)
three state model analysis tothe mean open time = 1/(b + g)
complications • Low Popen – difficult to know if you are analyzing a single channel • Low conductance – fluctuation analysis allows estimation of unitary conductance and mean open time • Subconductance levels NMDA receptor with pore loop mutation Premkumar et al. (1997) J Gen Physiol 109:181-189
Hodgkin Huxley kinetics • HH modeled Na current as a product of exponentials • Three independent activation gates (m) and one independent inactivation gate (h) • Compare this to the three state model where transit to C2 only occurs once the channel has opened
ball and chain model of inactivation See: Armstrong CM, Bezanilla F. (1977) J Gen Physiol. 70:567-90.
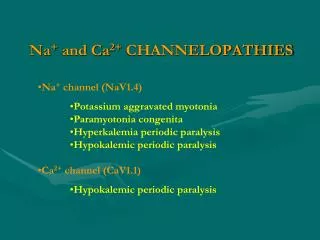
Ion Channel and Transporter Pathologies Diseases or syndromes caused by abnormal operation, distribution or regulation of channels or transporters • gain or loss of function mutations in ion channel genes (Channelopathies) • gain or loss of function mutations in auxiliary subunits • autoantibodies against channel protein • changes in assembly, trafficking or modulation Online Mendelian Inheritance in Man(https://omim.org/)
inherited or de novo Inherited channelopathies are relatively rare • exception: cystic fibrosis – a lung disease involving chloride channel mutations • 1/2000 are affected1/20 are carriers • DF508 – deletion of 3 base pairs encoding Phe 508 underlies 2/3 of cases world wide >90% of cases in the U.S. Zhang et al. (2017) Cell 170:483-491
genetic heterogeneity mutations to different genes similar phenotypes example: mutations to at least 11 different genes affect the QT interval • Long QT syndrome: KCNQ1, KCNH2, KCNE1, KCNE2, KCNJ2, KCNJ5 (LoF) CACNA1C, SCN5A, SCN4B (GoF) • Short QT syndrome: CACNA1C, CACNB2, CACNA2D1 (LoF)KCNH2, KCNQ1, KCNJ2 (GoF) Kim (2014) Korean J Pediatrics. 57:1-18.
dominant vs recessive different mutations to the same gene may be dominant or recessive • LoFrecessive; GoFlikely to be dominant • Haploinsufficiency – loss of one allele should reduce protein level by ~50%, which may be enough to alter phenotype • Dominant-negative mutations – the mutant copy adversely impacts the wild type copy (multimeric proteins)
KATP channels and insulin secretion Elevated blood glucose leads to a reduction in KATP channel activity in pancreatic b cells, increasing excitability and promoting insulin secretion • LoF mutants exhibit hyperinsulinemia and chronic low blood glucose • GoF mutants are neonatal diabetics with low insulin release and elevated blood glucose Colin Nichol’s labhttp://cimed.wustl.edu/
additional complexities • Phenotype may depend on genetic background • side effects of therapeutic drugs may involve acute or chronic changes in ion channels or transporters (kindling effect) • Autoantibodies – myasthenia gravis, anti-NMDA receptor encephalitis
Additional Reading • Hodgkin AL, Huxley AF. (1952) A quantitative description of membrane current and its application to conduction and excitation in nerve. J Physiol. 117:500-44. • Neher E, Steinbach JH. (1978) Local anaesthetics transiently block currents through single acetylcholine-receptor channels. J Physiol. 277:153-76. • Hoshi T, Zagotta WN, Aldrich RW. (1990) Biophysical and molecular mechanisms of Shaker potassium channel inactivation. Science. 250:533-8. • Zagotta WN, Hoshi T, Aldrich RW. (1990) Restoration of inactivation in mutants of Shaker potassium channels by a peptide derived from ShB. Science. 250:568-71. • Ashcroft FM. (2006) From molecule to malady. Nature. 440:440-7. • Kim JB. (2014) Channelopathies. Korean J Pediatrics. 57:1-18.