Download
1 / 65
801 likes | 1.14k Views
CAUSAL HETEROGENEITY IN ADHD: ARE THERE IMPLICATIONS FOR CLINICAL PRACTICE? . EDMUND SONUGA-BARKE. D. B. B L. Developmental Brain-Behaviour Laboratory. School of Psychology. OVERVIEW. DSM-IV ADHD subtypes – A successful way to handle heterogeneity? New approaches to ADHD subtyping.

E N D
CAUSAL HETEROGENEITY IN ADHD: ARE THERE IMPLICATIONS FOR CLINICAL PRACTICE? EDMUND SONUGA-BARKE D B B L Developmental Brain-Behaviour Laboratory School of Psychology
OVERVIEW • DSM-IV ADHD subtypes – A successful way to handle heterogeneity? • New approaches to ADHD subtyping. • Statistical refinement of the clinical phenotype. • Towards translational taxonometrics. • Neuropsychological markers of multiple causal pathways in ADHD. • Executive dysfunction • Delay aversion • Temporal processing • Implications: Treatment tailoring to subtype targets?
DSM-IV ADHD SUBTYPES – A SUCCESSFUL WAY TO HANDLE HETEROGENEITY?
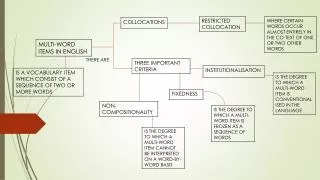
ADHD: THE CLINICAL REALITY Patients present with a range of clinical profiles with varying typesand degrees of; (i) symptoms of inattention, impulsivity/hyperactivity; (ii) comorbidity; (iii) complicating factors; and (iv) impairment. They may appear so different from one another that it is sometimes difficult to see them as having the same disorder. THE DIAGNOSTIC REIFICATION That this heterogeneity masks a core syndrome marked by a cluster of symptoms which can be distinguished from normality and from other related conditions and abstracted from local complicating factors and types of impairment.
HETEROGENEITY IN SYMPTOM PROFILE INATTENTION HYPER/IMPULSIVE
ATTENTION! SEVERITY Hyperactivity/Impulsivity Inattention
ADHD: THE CLINICAL REALITY Patients present with a range of clinical profiles with varying typesand degrees of; (i) symptoms of inattention, impulsivity/hyperactivity; (ii) comorbidity; (iii) complicating factors; and (iv) impairment. They may appear so different from one another that it is sometimes difficult to see them as having the same disorder. THE DIAGNOSTIC REIFICATION Heterogeneity masks a core syndrome category marked by a cluster of symptoms which can be distinguished from normality and from other related conditions and abstracted from local complicating factors and types of impairment.
HANDLING HETEROGENEITYIDENTIFYING SUBTYPES THE CREDIBILITY OF THIS CATEGORICAL VIEW DEPENDS ON OUR ABILITY TO PARTITION HETEROGENEITY IN CLINICALLY PLAUSIBLE WAYS. A number of approaches have been explored that address the putative causes of heterogeneity. • Gender – Are there separate male and female ADHD? • Severity and pervasiveness – ADHD vs HKD? • Familiality – Is ADHD different if it runs in the family? • Onset and persistence – Is adult onset a valid ADHD type? • Comorbidity – Is HK-CD a subtype or HKD with a comorbid condition? • Uneven symptom profile – Are differences between inattentive and hyperactive/impulsive types of aetiological and clinical significance?
DSM-IV SUBTYPES • 6 of 9 H/I • symptoms • 6 of 9 IA • symptoms H/I Type IA Type • 6 of 9 H/I & • 6 of 9 IA • symptoms Com Type ADDITIONAL DIAGNOSTIC CRITERIA Some symptoms/impairment before age 7 years; Some impairment in two or more settings ;Clinically significant impairment; Not accounted for by another disorder
THE VALUE OF DSM-IV SUBTYPES • Hyp/Imp and Inatt are overlapping but separate dimensions. • However subtypes.... • not stable over time • little genetic/familial specificity • poor neuropsychological discrimination • Little or no differential treatment response • Poor evidence for the validity of the ADHD subtypes. • HYP/IMP – PERHAPS A PRODROMAL FORM OF CT. • IA – PERHAPS SUB-THRESHOLD OR OTHER DISORDER. • Todd et al., 2008, McLoughlin et al 2007, Willcut et al, 2007, Gorman et al. 2006
THE FAILURE OF DSM-IV SUBTYPES: FUNDAMENTAL QUESTIONS. • Why ‘split’ rather than ‘lump’ anyway? To identify more homogenous causal entities that can be targeted more precisely -“get the right treatment to the right people”. • Can subtypes be refined to facilitate better treatment or should they be scrapped? • Can the clinical subtype be mapped more closely onto (i) the ‘causes’ of ADHD and (ii) treatment response? • Do we need to integrate ‘causal’ processes into subtypes? • Can this improve treatment? REFINE THE CLINICAL PHENOTYPE OR GO “DEEPER”?
NEW APPROACHES TO ADHD SUBTYPING. • 1, STATISTICAL REFINEMENT OF THE CLINICAL PHENOTYPE • 2. TOWARDS TRANSLATIONAL TAXONOMETRICS
REFINING THE CLINICAL PHENOTPYE • LATENT CLASS ANALYSIS Models the latent structure of the disorder on the basis of the manifest characteristics of ADHD patients.. …..to identify clusters of patients with distinctive clinical profiles….. …on the basis of (i) similarity of symptom endorsement and (ii) class prevalence. Dr Richard Todd PhD MD 2/17/1951-8/22/2008 Pioneer of latent class approaches to ADHD subtypes.
Rasmussen et al 2004 3-samples: Missouri Females Australian Females Australian Males 95% C.I.
DSM-IV SUBTYPES • 6 of 9 H/I • symptoms • 6 of 9 IA • symptoms H/I Type IA Type • 6 of 9 H/I & • 6 of 9 IA • symptoms Com Type ADDITIONAL DIAGNOSTIC CRITERIA Some symptoms/impairment before age 7 years; Some impairment in two or more settings ;Clinically significant impairment; Not accounted for by another disorder
Few symptoms LATENT CLASS REFINEMENT Mild Inattentive Talkative Impulsive Inattentive/Impulsive Severe Hyper/Impulsive Severe Inattentive Combined Severe Rasmussen et al 2004
THE VALUE OF LATENT CLASS SUBTYPES • Replicable and robust (Rasmussen et al., 2004). • Identify previously overlooked types (mild CT; Volk et al., 2006). • Are systematically/differentially related to impairment – severe IA, severe CT, moderate CT are most impaired (Volk et al., 2006). • A little more stable over time than DSM-IV types (Todd et al., 2008). • Is stable across informants (Alhoff et al., 2006). • May help us to understand the overlap with comorbid conditions. • ODD/CD (Acosta et al., 2008) • Autism (Reiersen et al., 2007) • Developmental Co-ordination Disorder (Reiersen et al., 2008). • Can be operationalised as simple diagnostic rules (Volk et al., 2009) . • May be more aetiologically homogenous – map clinical phenotype more closely on causal pathways. • More heritable (Todd et al., 2001). • Linked to specific measured genes and environments (Neuman et al., 2007).
CAN WORKING ONLY AT THE LEVEL OF THE CLINICAL PHENOTYPE EVER ALLOW US TO IDENTIFY HOMOGENEOUS CAUSAL ENTITIES?
LATENT CLASS REFINEMENT OF CLINICAL PHENOTYPE Mild Inattentive Talkative Impulsive Inattentive/Impulsive Severe Hyper/Impulsive Severe Inattentive Combined Severe Rasmussen et al 2004
SIMPLE CLINICAL PHENOTYPE CAUSE MODEL If you can refine the clinical phenotype sufficiently you will produce a 1:1 map to cause. Cause X Cause Y Cause Z
COMPLEX CLINICAL PHENOTYPE-CAUSE MODEL Causes remote from clinical phenotype. Equi-finality and multi-finality in causal pathways. 1:1 match between clinical phenotype and cause impossible. Cause X Cause Y Cause Z
INTEGRATING CAUSAL FACTORS INTO SUB-TYPE MODELS • TOWARDS TRANSLATIONAL TAXOMETRICS Shifts the focus from manifest variables (exophenotype) to markers of neuro-biological processes (endophenotype)… …to identify subgroups of patients whose ADHD have distinctive “causes”… …which can promote the tailoring of new treatments to new treatment targets. • BUILT ON CAUSAL PATHWAY MODELS OF ADHD
NEUROPSYCHOLOGICAL MARKERS OF MULTIPLE CAUSAL PATHWAYS IN ADHD • EXECUTIVE DYSFUNCTION • DELAY AVERSION • TEMPORAL PROCESSING
THE BIO-MEDICAL MODEL HAS PROMOTED A MODEL OF CAUSAL HOMOGENEITY A reified disease-based notion of disorder is insufficiently grounded in the reality of the patient population. • Mental Disorders are: discrete • dysfunctional/endogenous/trait-like/homogenous Where is the fixed-common core dysfunction in the brains/minds of ADHD children that ‘causes’ the disorder?
WHAT IS THE CORE DEFIT? Originating Causes Neuro- biological Alteration Neuro- psychological deficit Disorder
EXECUTIVE DYSFUNCTION MODEL Executive CircuitThalamo-cortico-striatal loop A Simple Cognitive Deficit Model PRIMARY MOTOR AREA DA NE EXECUTIVE CIRCUIT DISTURBANCE DLPFC GENERALISED EXECUTIVE DEFICITS THALAMUS DORSAL STRIATUM Caudate Nucleus ADHD DA Adapted from Barkley, 1997 Adapted from Alexander, 1986
THE NOTION OF A STABLE CORE DEFICIT IS A SCIENTIFIC RED HERRING Solid evidence base Links EDF and its neural substrate & ADHD. • Deficits in working memory, attentional flexibility, planning • Inhibitory deficits may be a precursor • Evidence implicating... • pre-fronto-striatal networks • dopamine, norepinephrine (Genes, Drugs) Executive dysfunction is not the common core fixed deficit that ‘causes’ ADHD. Not the Holy Grail for which we have been searching.
EXECUTIVE DYSFUNCTION: A NECESSARY & SUFFICIENT CONDITION FOR ADHD? But… only a proportion of children with ADHD have EDF. many children without ADHD have EDF. EDF in ADHD nearly always presents in partial and fragmented way.
IF NOT EXECUTIVE DYSFUNCTION WHAT THEN? Most children with ADHD don’t show executive dysfunction. What ‘causes’ ADHD in these other cases? ? Proportion of ADHD children with a broad-based EF deficit (equivalent to 10 percent controls) DO TEMPORAL PROCESSING DEFICITS AND DELAY AVERSION REPRESENT ADDITIONAL ‘CAUSES’ WHICH ARE DISSOCIABLE FROM EXECUTIVE DYSFUNTION?
DISSECTING HETEROGENEITY IN ADHD: DELAY SENSITIVITY, EXECUTIVE FUNCTIONING AND TEMPORAL PROCESSING. Bitsakou, Temporal Sonuga-Barke (submitted) To examine the independence and overlap of temporal processing, executive function and delay aversion components to ADHD.
NINE NEUROPSYCHOLOGICAL TASKS • INHIBITORY CONTROL • Stop Signal Adjusted to 50% correct SSRT • Go-NoGo G – left or right arrow NG – double headed arrow Probability of inhibition • Stroop-like Compatible – green arrows Conflict – red arrows Probability of inhibition • DELAY SENSITIVITY • MIDA • 1pt – 2-s:: 2pt – 30-s No post reward delay Choice of LL • Delay Frustration 55 simple problems 8 x 20-s.imposed delay Responses during to delay • Delayed Response Press when arrow disappears No delay Delay 3-s and 20-s (RT delay – RT immediate) • TEMPORAL PROCESSING • Discrimination • Target 400ms tone Comparator adjusted by 10 ms Average time difference between tones • Reproduction Target interval signalled Target invisible not signalled RT non-signal trials • Tapping Tap to regular tone (1200ms) Tap no tone Variability on no tone trials Working memory (digit span) and IQ also collected
ALL 4 DOMIANS ARE ASSOCIATED WITH ADHD. FACTOR SCORE (STANDARIDZED) I-EDF NEID PUD TPD
PROPORTIONS WITH DEFICIT AND OVERLAP DELAY n=25 15 (19.5%) 1 (1.6%) EF n=16 4 (5.2%) 5 (6.4%) 5 (6.5%) NO DEFICIT n=22 6 (7.8%) 19 (24.%) TIME n=34 Based on 10% cut in normals
SIMPLIFIED FUNCTIONAL NEUROANATOMY OFC MOTOR CORTICES CORTICO-VENTRAL STRIATAL LOOP DISTURBANCE CORTICO-DORSAL STRIATAL LOOP DISTURBANCE CORTICO- CEREBELLAR LOOP DISTURBANCE ANTERIOR CINGULATE DLPFC TEMPORO-SENSORY-MOTOR INTEGRATI’N DEFICITS IMPAIRED SIGNAL DELAYED REWARD INHIBITORY DEFICITS THALAMUS AMYGDALA VENTRAL STRIATUM Nucleus Accumbens DORSAL STRIATUM Caudate Nucleus DELAY AVERSION EXECUTIVE DEFICITS MOTOR ASYNCHRONY ADHD NEO CEREBELLUM A TRIPLE PATHWAYHYPOTHESIS
IMPLICATIONS FOR PRACTICE • DIAGNOSTIC IMPLICATIONS: SHOULD THERE BE CAUSAL SUBTYPES MARKED BY NEUROPSYCHOLOGICAL DEFICITS? • EDF, DEL & TD .. • as epiphenomenon • as subtypes of disorder • as complication & comorbidity
SHOULD WE MODEL PHENOTYPIC AND ENDOPHENOTYPIC HETEROGENEITY SIMULTANEOUSLY?
SHOULD WE MODEL PHENOTYPIC AND ENDOPHENOTYPIC HETEROGENEITY SIMULTANEOUSLY? Impulsive /Inattentive Timing Impulsive/ Inattentive Executive Impulsive-Inattentive Delay Averse. Combined Severe - Timing Combined Severe - Executive Combined Severe – Delay Averse
OR SHOULD WE SEE DEFICITS AS EXTENDED ACROSS DISORDER TYPES?: A COMPLICATION RATHER THAN A SUB-TYPE EDf DAv TimD
OR SHOULD WE SEE DEFICITS AS EXTENDED ACROSS DISORDER TYPES?: A COMPLICATION RATHER THAN A SUB-TYPE EDf DAv ADHD TimD
PDD ODD/CD EDf DAv ADHD Dyslexia/LD TimD OR SHOULD WE SEE DEFICITS AS EXTENDED ACROSS DISORDER TYPES?: A COMPLICATION RATHER THAN A SUB-TYPE
IMPLICATIONS FOR PRACTICE • DIAGNOSTIC IMPLICATIONS: SHOULD THERE BE NEUROPSYCHOLOGICAL SUBTYPES? • EDF, DEL & TD .. • as epiphenomenon • as subtypes of disorder • as complication & comorbidity • TREATMENT IMPLICATIONS CAN WE DEVELOP NEW TREATMENTS TO TARGET SPECIFIC ‘CAUSAL’ SUBTYPES. • Treatment • Develop new treatments to target specific pathways. • Pharmacological • Psychological • Target/tailor treatments more effectively. • Assessment • Biological/psychological markers • The role of context
MEDIATORS OF SPECIFIC PATHWAYS ARE POTENTIAL THERAPEUTIC TARGETS Originating Causes G, E, GxE Neuro- biological alteration Neuro- psychological deficit Disorder
IDENTIFYING SUCH DEFICITS SHOULD BE A STIMULUS FOR PHARMACO-THERAPEUTIC INNOVATION Originating Causes G, E, GxE Medication Altered circuits Deficits Disorder
MAJOR DOPAMINE & NOREPINEPHRINE BRANCHES OFC DLPFC MOTOR CORTICES VENTRAL STRIATUM Nucleus Accumbens DORSAL STRIATUM Caudate Nucleus NEO CEREBELLUM
MEDIATORS OF DISEASE PROCESSES REPRESENT POTENTIAL THERAPEUTIC TARGETS Originating Causes G, E, GxE Neuro- biological alteration Neuro- psychological deficit Disorder
IDENTIFYING SUCH PROCESSES SHOULD BE A STIMULUS FOR PSYCHO-THERAPEUTIC INNOVATION Originating Causes G, E, GxE Neuro- biological alteration Neuro- psychological deficit Training Disorder