Download
1 / 43
430 likes | 512 Views
Breath Tests, pH-Metry and Impedance. Michael J. Lentze Zentrum für Kinderheilkunde University Hospitals Bonn Oct 2013. Clinical Use of H 2 -Breath Test. Ghoshal UC J Neurogastroenterol Motil 17: 312-17, 2011. Typical Exhalation Curves in CH H 2 -Breath Tests.

E N D
Breath Tests, pH-Metry and Impedance Michael J. Lentze Zentrum für Kinderheilkunde University Hospitals Bonn Oct 2013
Clinical Use of H2-Breath Test Ghoshal UC J Neurogastroenterol Motil 17: 312-17, 2011
Typical Exhalation Curves in CH H2-Breath Tests Ghoshal UC J Neurogastroenterol Motil 17: 312-17, 2011
Clinical Use of H2-Breath Test Substrate Utility Glucose H2-breath test Glucose Small intestinal overgrowth Glucose malabsorption Lactulose H2-breath test Lactulose Oro-cecal transit time Small intestinal overgrowth Lactose H2-breath test Lactose Lactose malabsorption Fructose H2-breath test Fructose Fructose malabsorption Sucrose H2-breath test Sucrose Sucrase-Isomaltase Defiency
Clinical Case: 10 year old Boy • Healthy until his 6 th year of life, than episodes of vomiting and diarrhea • These episodes occur in intervals of weeks • When diarrhea occurs he had 17-20 liquid stools per day • During these episodes he lost weight • In between episodes he was completely normal and healthy • During the last episode he had a complete workup in the refering hospital. Normal: red and white blood count, BSR, liver transaminases, creatinine, TTG-antibodies, H2-Lactose breath test, sonography of abdomen, coloscopy, histology, upper GI-series • It was suggested to the parents to see a child psychologist • Before he was refered for a second opinion to us
Nutrition • The boy’s nutrition consisted in: • Morning: Milk, cornflakes, honey, bred with marmelade • Noon: from the table, in addition plenty of fruits, drinks Coca-Cola • Afternoon: Chocolate, Fruitcake • Dinner: bred, salad, fruits • When I asked his brother whether he also liked sweets and fruits, he answered: yes, but his brother was eating up everything , so nothing was left for himself
Genetic Variant of Adult Hypolactasia on Chromosome 2q21 8 kb 14 kb Promot Lactase-Phlorizin Hydrolase C/C - 13910 Function? G/G - 22018 Found in 229/236 cases from Finland, Germany, Italy, Korea Enattah NS et al Nat Genet 30: 233, 2002
Adult Hypolactasia Ratio Lactase/Sucrase Expression of Lactase Gene Kokkanen M et al Gut 52: 647-52, 2003
Decline of Lactase in C/C-13910 Individuals Finnish Children African Children Rasinperä H et al Gut 53: 1571-76,2004
Phenotype- Genotype-Correlation A-22018 C-14010 G-13915 G-13907 Tishkoff SA et al, Nature Genet 39: 31-40,2007
Malabsorption of Lactose and Fructose and RAP 220 children with RAP had Lactose and Fructose H2-Breath Test (double blind testing): Lactose-Malabsorption 57/210 Fructose-Malabsorption 79/121 Pain disappeared (Lac-Malabs) 24/38 Pain disappeared (Fruc-Malabs) 32/49 Open provocation + Lact.: positive 7/23 Open provocation + Fruct.:postive 13/31 Conclusion: Neither Lactose- nor Fructose intolerance could be established as cause for RAP Gijsbers CFM et al 2012
Secondary Lactose Intolerance in PEM • 196 severely malnourished childen Lactose intolerance in 50 children (25%): • 27/75 with Kwashiorkor • 6/25 Marasmic Kwashiorkor • 17/96 Marasmus Assessment: stool ph, reducing substances in stool Nyeko R et al. BMC Pediatrics 10:31, 2010
Interaction of Hydrolysis and Absorption of Glucose and Fructose Intestinal Lumen Brush Border Membrane Cytoplasm Sucrose Sucrase-Isomaltase Glucose SGLT1 Na+ + + Fructose GLUT5 + Glycin Na+-GlycineTransporter Na+
Age Dependency of Fructose and Lactose Intolerance Lactose H2-BT Fructose H2-BT Jones HF JPGN 52:581-84, 2011
Lactose Intolerance in IBD Relationship between Symptoms and Genotype Eadala P et al. Aliment Pharmacol Ther 34: 735-46, 2011
13C-Urea Breath test for the Diagnosis of H.pylori Infection in Children- Meta-Analysis Children 6 years and younger 95% 94% Leal YA et al. Helicobacter 16:327-37, 2011
13C-Urea Breath test for the Diagnosis of H.pylori Infection in Children- Meta-Analysis Children 6 years and older 97% 98% Leal YA et al. Helicobacter 16:327-37, 2011
Prevalence of H.pylori Infection in a Population:36.629 People in Denmark by Home 13C-Breath Test Dahlerup S et al. Helicobacter 16: 468-74, 2011
Age and Gender Differences in H.P. Breath Tests Zevit N et al Eur J Clin Invest 41: 767-72,2011
Shall we use 13C Urea Breath Test for the Diagnosis of RAP? The test would applicable, if the symptoms would correlate to positive findings, but there is no correlation between RAP and H.P.-Infection Spee LAA et al. Pediatrics 125: 651-69, 2010
H. pylori Antigen in Stool Guarner J et al. Eur J Pediatrics 169: 15-25, 2010
ESPGHAN-NASPGHAN Guidelines for the Management of H.pylori Infection 1. For the diagnosis of H. pyloris infection during EGD, it is recommended that gastric biopsies (antrum and corpus) for histopathology be obtained 2. It is recommended that the initial diagnosis of H.p. be based on either histopathology plus positive rapid urease test or a positive culture 3. The 13C-urea breath test is a reliable noninvasive test to determine whether H.p. has been eradicated. 4. A validated ELISA test for detection of H.p. in stool is a reliable noninvasive test to determine whether H.p. has been eradicated 5. Test based on the detection of antibodies (IgG, IgA) against H.p. in serum, hwole blood, urine and saliva are not reliable for use in the clinical setting Koletzko S et al. JPGN 53: 230-243, 2011
Algorithm for Treatment of H.pylori Infection in Children Koletzko S et al. JPGN 53: 230-243, 2011
Has the 13C-Urea Breath Test a Future? 13CO2 13C-Urea M.tuberculosis Urease + NH3
High Burden Countries for Tuberculosis Maiga M et al. Indian J Med Res 135: 731-36, 2012
Rabbits infected with M. tuberculosis 13C-Urea Breath Test Maiga M et al. Indian J Med Res 135: 731-36, 2012
Predicted Outcome of Breath Test for active Tuberculosis Philipps M et al. Tuberculosis 92: 414-20, 2012
Utility of 13C-Breath Tests Braden B Best Pract Res Clin Gastroenterol 23: 337-52, 2009
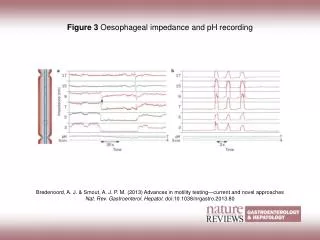
Multichannel intraluminal Impedance And pH-Metry Wenzl, T. G. et al. Pediatrics 2003;111:e355-e359
Detection of GER in 700 Children using Multichannel Intraluminal Impedance (MII) and pH-Metry Number of abnormal Measurements Pilic D et al. J Pediatrics 158: 650-4, 2011
Arguments pro MII-pH-Metry • MII + pH- is most sensitive method to detect acidic, weakly acidic and alkaline refluxes • Is the best method to correlate symptoms with reflux events • Diagnostic gain for combining the 2 methods is 22% - 32% • MII detects the proximal extent of refluate which is important for increased risk of aspiration • In children with asthma it can show also weakly acidic refluxes (51%) • In preterm infants apnea episodes occur more frequently after a reflux event of which 57% are non-acidic. • Outcome studies are lacking Blondeau K et al Am J Gastroenterol 104: 3664-6, 2009
Arguments contra MII-pH-Metry • What does an non-acid reflux mean? • Automated detection overestimates the number of reflux episodes • More difficult to read • Nasal catheter is uncomfortable • Outcome studies are missing, e.g. after fundoplication Richter JE Am J Gastroenterol 104: 2667-69, 2009
Intraobserver Variability in MII + pH Metry • 10 experienced observers in the world had to read 1242 liquid and mixed GER • 490 GER were scored by all observers = 42% !! • Agreement for gas GER was poor • Automated analysis was better than that of observers • Widespread use cannot be advocated at present Loots CM et al. J Pediatrics 160: 441-6, 2012
Reflux Events by pH-MMI do not determine Fundoplication Outcome Rosen R et al. JPGN 50: 251-255, 2010
Reflux Events by pH-MMI do not determine Fundoplication Outcome Rosen R et al. JPGN 50: 251-255, 2010
Diagnostic Steps in GERDfor an Infant with recurrent Regurgitation and vomiting Evaluate further Evaluate further ESPGHAN-NASPGHAN guidelines JPGN 49: 498-547, 2009
Diagnostic Steps in GERDfor an Infant with recurrent Regurgitation and Weight Loss ESPGHAN-NASPGHAN guidelines on GERD JPGN 49: 498-547, 2009
Diagnostic Steps in GERDfor an older Child or Adolescent with Heartburn ESPGHAN-NASPGHAN guidelines on GERD JPGN 49: 498-547, 2009
Diagnostic Steps in GERDfor a Child with Asthma that might be worsened by GERD ESPGHAN-NASPGHAN guidelines on GERD JPGN 49: 498-547, 2009
Recommendation for Treatment of GERD ESPGHAN-NASPGHAN guidelines on GERD JPGN 49: 498-547, 2009 • In infants try extensively hydrolysed formula for 2-4 weeks (Eosinophilic Esophagitis?) • Thicken formula • Supine position during sleep • In adolescents with GERD left-side sleeping and elevation of the head decreases GERD • PPI‘s are more effective than H2RAs • Insufficient support for metoclopramide, erythromycin, bethanechol or domperidone • Buffering agent as sucralfate, alginates are not recommended • Antireflux surgery should only be considered in failure of optimized medical therapy or life-threatening complications