Download
1 / 50
570 likes | 1.14k Views
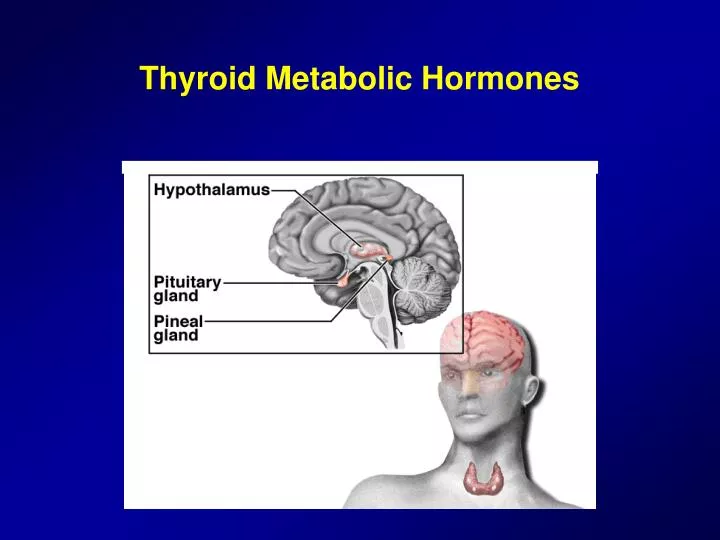
Thyroid Metabolic Hormones. Hypothalamo-Hypophyseal-Thyroid Axis. Hormones in regulation of thyroid metabolism. TRH (Hypothalamus) TSH (Anterior pituitary) T3 and T4 (Thyroid gland). Thyroid Gland. Location of Thyroid Gland.

E N D
Hormones in regulation of thyroid metabolism • TRH (Hypothalamus) • TSH (Anterior pituitary) • T3 and T4 (Thyroid gland)
Location of Thyroid Gland • It is located in the anterior wall of trachea, just below the larynx • It is composed of two lobes which are joined at the isthmus
Colloid Follicle Epithelial cells Histology of Thyroid Gland - I
Histology of Thyroid Gland - II • Active Gland • Columnar epithelium • Reduced colloid • Inactive Gland • Cuboidal epithelium • Increased colloid
Iodine is Required for Formation of Thyroxine • To form normal quantities of thyroxine, about 1 mg of iodine should be ingested per week • Iodides are absorbed from the GI tract into the blood • Most of the iodides are excreted by the kidneys • 1/5 is taken up by the cells of thyroid gland for synthesis of T3 and T4
Iodide Pump (Iodide Trapping) • The basal membrane of the thyroid cells has a specific ability to pump iodide actively to the interior of the cell. This is called iodide trapping. • The rate of iodide trapping by the thyroid is influenced by several factors • TSH stimulates and hypophysectomy greatly reduces the activity of iodide pump in thyroid cells
Thyroglobulin • Thyroid cells synthesize a glycoprotein (thyroglobulin) and secrete into the follicle • Each thyroglobulin contains about 70 tyrosine aa • Thyroid hormones are stored as attachment to thyroglobulin molecule in the colloid
Oxidation of the iodide ion • The first essential step in the formation of the thyroid hormones is conversion of the iodide ions to an oxidized form of iodine • Iodized iodine (I3-) is capable of combining with thyrosine • This oxidation is promoted by peroxidase and accompanying H2O2 • When the peroxidase system is blocked, thyroid hormones cannot be synthesized
Cell Extracellular space T.P. + H2O2 I I I I I I I I Colloid I I I THYROGLOBULIN I* I I - I + T.P. + H2O2 T3,T4 A.A. - I
Iodination of tyrosine and formation of thyroid hormones • Oxidized iodine first binds to the thyroglobulin (organification of the thyroglobulin) • Iodines then bind with tyrosine amino acids • Role of iodinase enzyme • Monoiodotyrosine, diiodotyrosine …
I 5 5’ O HO CH2 CH COO- 3’ 3 I I T3 = 3,5,3’-L-triiodothyronine NH3+
I I 5 5’ O HO CH2 CH COO- 3’ 3 I I T4 = 3,3’,5,5’-L-tetraiodothyronine(thyroxine) NH3+
Release of Thyroid Hormones from the Thyroid Gland • Normally thyroglobulin is not released into blood • T3 and T4 are cleaved from the thyroglobulin and secreted into the blood • Interaction of thyroglobulin with lysosomes • Proteases digest thyroglobulin and release T3 and T4 in free form
Daily rate of secretion of thyroxine and triiodothyronine • About 93% of the thyroid hormne released from the thyroid gland is normally thyroxine (T4) • and only 7% is triiodothyronine (T3) • However, the hormone finally delivered to and used by the tissues is mainly T3
Transport of T3 and T4 to Tissues • On entering the blood, almost all of T3 and T4 combines with plasma proteins, mainly globulins • T4 and T3 are released slowly to tissue cells • Thyroid hormones have slow onset and long duration of action
Mechanism of Thyroid Hormone Actions • Slow onset and long duration of action • Rapid action: T3 (small amount); Slow action: T4 • They bind their nuclear receptors and stimulate gene transcription • They increase number and activity of mytochondria • They also stimulate synthesis of Na-K ATPase and ion transport through the cell membrane
Effects of Thyroid Hormones on Growth • They are essential hormones for growth • They strongly stimulate metabolism • The effects of thyroid hormones on growth manifest mainly in growing children • They promote growth and development of the brain during fetal life and for the first few years of postnatal life (mental deficiency, cretenisim).
Metabolic Effects - I • They stimulate all aspects of carbohydrate metabolism (glucose uptake, enhanced glycolysis, increased gluconeogenesis, increased absorption) • They increase fat metabolism. Stimulate oxidation of fatty acids in cells and mobilization of lipids as energy source • Increased thyroid activity increases plasma levels of fatty acids, but reduces cholesterol, phospholipid and triglycerides • They normally stimulate protein synthesis, but excessive activity causes catabolism of proteins
Metabolic Effects - II • Increased requirement for vitamins • Increased basal metabolic rate and decreased body weight • Effects on cardiovascular system • Stimulation of respiration • Increased gastrointestinal motility • Excitatory effects on the CNS • Effect on the function of muscles • Effect on sleep • Effects on other endocrine glands and sexual functions
TRH stimulation of thyrotropic cells in the anterior pituitary which secrete TSH TRH binds its specific receptors on the thyrotrops It uses phospholipase second messenger system Phospholipase C
Cellular Effects of TSH • TSH binds its specific receptors on the thyroid cells in the thyroid gland • It activates cAMP as second messenger system
TSH Increases Thyroid Secretion • Increased proteolysis of thyroglobulin • Increased activity of iodide pump • Increased iodination of thyrosine • Increased size and secretory activity of the thyroid cells • Increased number of thyroid cells and a change from cuboidal to columnar cells
Histology of Thyroid Gland - II • Active Gland • Columnar epithelium • Reduced colloid • Inactive Gland • Cuboidal epithelium • Increased colloid
Antithyroid Substances • Thiocyanate ions decrease iodide trapping: Decreased availability of iodide in the glandular cells does not stop formation of thyroglobulin. TSH stimulates outgrowth of the thyroid gland even though the gland still does not form adequate quantities of thyroid hormones (goiter) • Propylthiouracil (PTU) decreases thyroid hormone formation. PTU prevents formation of thyroid hormones from iodide and tyrosine. They partly block the enzymatic activity of peroxidase and also prevent coupling of two iodinated tyrosines to form T3 and T4. • Iodide in high concentrations decrease thyroid activity and thyroid gland size. They reduce rate of iodide trapping and endocytosis of colloid from the follicle is prevented. Depot thyroglobulin cannot release T3 and T4 into the blood.
Hyperthyroidism • Causes of hyperthyroidism (Toxic goiter, thyrotoxycosis, Graves’ Disease) • Activity of the thyroid gland is greatly increased • Plasma TSH levels are reduced in RIA • Thyroid-Stimulating Immunoglobulin (TSI) is similar to TSH and binds to the same receptors. TSI also stimulates the thyroid gland • TSI antibodies are formed as a result of autoimmunity against to the thyroid tissue • TSI increases release of T3 and T4 which in turn reduces hypophyseal TSH by negative feedback mechanism
Hyperthyroidism Exophthalmus Goiter Columnar thyroid cells
Symptoms of Hyperthyroidism • Exophthalmus • A high state of excitability • Intolerance to heat • Increased sweating, weight loss, sometimes diarrhea • Muscle weakness, tremor in hands • Nervousness or other psychic disorders • Extreme fatigue but inability to sleep
Diagnostic tests for hyperthyroidism • The most accurate diagnostic test is direct measurement of free T4 levels in plasma • Plasma TSH levels are reduced • Presence of TSI should be examined • Hashimoto's disease is an autoimmune disorder in which immune system inappropriately attacks the thyroid gland, causing damage to the thyroid cells (inflammation)
Physiology of treatment in hyperthyroidism • Surgical removal of the most of the gland • Administration of PTU to patients for several weeks • reduction of basal metabolic rate • Then, administration of high concentrations of iodides for 1 to 2 weeks • Reduced gland size and blood hormone levels • Operation • Use of radioactive iodine in hyperplastic (hyperplasia) thyroid gland
Hypothyroidism • Endemic goiter caused by dietary iodide deficiency: Iodide deficiency decreases synthesis of T3 and T4 but formation of thyroglobulin in the colloid continues. Excessive TSH greatly stimulates the thyroid gland • Idiopathic nontoxic goiter • release of hormone is reduced • Most of such patients show mild thyroiditis • Some foods contain goitrogenic substances that have a PTU-type of anti-thyroid activity (turnips and cabbages)
Physiologic Characteristics of Hypothyroidism • Myxedema develops because of excessive quantities of hyalurinic acid and chondroitin sulfate in the interstitial space • Atherosclerosis in hypothyroidism (increased plasma levels of cholesterol and diminished excretion of it by the liver) • Basal metabolic rate is decreased • Plasma T3 and T4 levels are reduced • Exogenous TRH administration greatly increases TSH • Treatment with administration of T4 (thyroxine)
Cretinism • Caused by extreme hypothyroidism during fetal life, infancy or childhood • Mental retardation • This results from retardation of the growth, branching and myelination of the neurons in the CNS at the critical period • Skeletal growth in the child with cretinism is charteristically more inhibited than is soft tissue growth