Download
1 / 25
250 likes | 348 Views
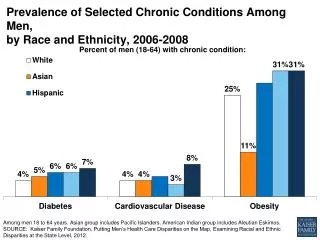
Prevalence of chronic conditions in Wales from the Quality and Outcomes Framework. August 2011. Presenter: Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS). Aims and objectives of the report.

E N D
Prevalence of chronic conditions in Wales from the Quality and Outcomes Framework August 2011 Insert name of presentation on Master Slide Presenter: Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS)
Aims and objectives of the report • Provide assistance to explore the potential use of Quality and Outcomes Framework (QOF) data to describe chronic condition prevalence across Wales. • It seeks to: • describe the prevalence of key chronic conditions as recorded by general practice QOF registers at health board and local authority levels • improve our understanding of QOF prevalence by • examining variation of prevalence at practice level across Wales • examining the association with deprivation at practice level • set these findings in context Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
What did we do ? • Provide the QOF direct age standardised and crude rates for local health board and local authority areas • Provide a view of the Wales GP practice, QOF direct age standardised prevalence • Provide the GP practice, QOF direct age standardised prevalence correlated with deprivation (Townsend) to indicate if there is a correlation or association between the two. • Provide the Welsh age standardised Welsh Health Survey (WHS) prevalence at health board and local authority area to act as a cross reference Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Some important considerations • Age standardisation • The actual recorded prevalence of the conditions is the ‘crude’ prevalence. • it can be misleading when comparing different populations. In particular, disease and mortality rates vary with age. • Age-standardisation allows comparison of rates across different populations while taking account of the different age structures of those populations. Example of varying practice population age structures Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Some important considerations • Confidence intervals • Confidence intervals are indications of the natural variation that would be expected around the prevalence and they should be considered when assessing or interpreting the prevalence. • The size of the confidence interval is dependent on the number of events occurring and the size of the population Example of varying confidence intervals for practices localities and former LHB Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Source of the data • Data extract from Audit +/Audit web as at march 2010 • GP practice deprivation scores will use Townsend 2001 and the distribution of practice populations as at 2006 • Welsh Health Survey 2008 - 2009 Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Data availability and quality • QOF data is primarily used to monitor GP practice performance against their contract; secondary uses of data need interpretation with caution. • QOF data can now be age standardised allowing improved comparisons of QOF prevalence. • The quality of QOF data has improved through a number of data quality initiatives and coding specifications. The conditions included in this report have substantial data maturity. Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Some important considerations • Data caveats • It is unclear as yet how analysis of this data for a secondary purpose approximates to the true prevalence of the conditions examined. • Return rate 90% overall however variable return rates locally • Recording data in the community Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Some important considerations Coding Issues examples H/O asthma and an asthma related prescription in the 12 months but no diagnostic code of Asthma CABG Read code in notes but no CHD diagnostic code No episode type with Depression. To count in depression register you must have a F (first) or N (new) episode type associated with the diagnostic code A diagnostic diabetic Read code in notes but not one indicating Type 1 (C10E..) or Type 2 (C10F..) which puts a patient on the QOF register Stroke/TIA monitoring Read code in notes but no diagnostic read code A diagnostic COPD Read code that are not included in the QOF Read codes for a COPD register Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Findings Headline crude rates for diagnosed conditions2.0% Stroke TIA4.1% coronary heart disease14.9% hypertension4.8% diabetes6.6% asthma2.0%COPD Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Findings - Variability in prevalence • There is substantial variability of QOF prevalence of chronic conditions. This is, as expected, greater between local authorities than between health boards. • The variability is more dramatic at GP practice level, • many practices have a prevalence in excess of three standard deviations either above or below the Welsh mean. • 8% (stroke/TIA) to 52% (hypertension) of Welsh GP practices. • The least variability conditions with an onset that is easily recognised by both the patient and clinician, e.g. stoke/TIA, and • greatest for conditions where identification is more dependent on individual and clinician practice, e.g. hypertension. • This variability beyond what might be expected by chance is not explained by age and would benefit from further investigation. Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Results – variation –Stroke TIA The age standardised prevalence ranges from 1.2% to 1.4% of the registered population, compared to a Wales average rate at 1.3%. Crude prevalence figures show more variation ranging from 1.7% to 2.2% compared to a Wales average at 2.0%. Dramatic variation across general practice QOF recorded hypertension, even after accounting for age. Eight per cent of practices lie outside the expected (three standard deviation) range. The Range from 0.4% to 2.3% percent of the population. over dispersion suggesting underlying systematic factors, other than age, that may need to be taken into account when considering the distribution of practices around the Welsh mean. The range is 1.0% to 1.6% of registered patients. Crude rates again show more variation ranging from 1.6% to 2.6% of registered patients. Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Results – variation – Hypertension Dramatic variation Fifty-two per cent of practices lie outside the expected (three standard deviation) range. The Range from 3.2% to 20.0% percent of the population. substantial over dispersion suggesting underlying systematic factors, other than age, that may need to be taken into account when considering the distribution of practices around the Welsh mean. The age standardised prevalence ranges from 10.2% to 12.9% of the registered population, compared to a Wales average rate at 11.1%. Crude prevalence figures show more variation ranging from 12.4% to 16.4% compared to a Wales average at 14.9%. The range is 8.8% to 13.3% of registered patients. crude rates show more variation ranging from 11.5% to 17.5% of registered patients.
Findings - Geographical patterns of prevalence • The QOF prevalence of diagnosed chronic conditions shows broadly an expected geographical pattern, • higher prevalence in more deprived areas such as Cwm Taf and • lower prevalence in less deprived areas such as Powys. • Some consistency in the relative position of health board and local authority areas between QOF and the Welsh Health Survey (WHS). • Some inconsistent such as • relatively low prevalence of diagnosed stroke or transient ischaemic attack (TIA) in Blaenau Gwent, • relatively low prevalence of diagnosed asthma in Cwm Taf • relative position for asthma and COPD inconstant with WHS in Carmarthenshire Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Geographical patterns of prevalence - health board comparison Stroke QOF v WHS Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Geographical patterns of prevalence - local authority area comparison Stroke QOF v WHS Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Geographical patterns of prevalence - health board comparison Hypertension QOF v WHS Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Geographical patterns of prevalence - local authority area comparison Hypertension QOF v WHS Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Findings Deprivation V Prevalence • Many conditions demonstrate the expected association with deprivation, although this association is weak • Calculation of practice deprivation scores may underestimate the correlation as practice catchment populations span areas of mixed deprivation levels • It can also highlight pockets of deprivation where a single practice may serve one specific area of deprivation in, an otherwise affluent area. • Student populations demonstrate deprived characteristics through the Townsend index. Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Variation in Practice Deprivation Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Deprivation V Prevalence Hypertension Stroke/TIA In this instance the co-efficient value for Wales is 0.23 Although this association is statistically significant, it is so weak it falls into the little or no association grade In this instance the co-efficient value for Wales is 0.35, Although this association is statistically significant, it shows a weak positive correlation or association Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Conclusions - general • Audit+ and Audit web software have allowed access to data to calculate age standardised, diagnosed prevalence data for various conditions from GP practices across Wales covered by the QOF. (with some caveats) • The software is installed in 97% of Welsh practices, with monthly return rates of around 90%. • Caution required in using the data • data is collected for contract monitoring and not specifically for the monitoring of Public Health. • Prevalence may not reflect the true prevalence as there is variability in the capture of data into IT clinical systems due to varying GP practice and clinician preference. Coding and data quality issues Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Conclusions from results • QOF age standardised rates generally • show a weak correlation with deprivation • follow an expected geographic pattern i.e. higher where deprivation is higher and lower where deprivation is lower, with some exceptions e.g. Carmarthenshire for Asthma and COPD, • The utility of QOF data may be improved from its early years. • Variability at GP practice level is considerable • Increasing where conditions are less easily identified. • Age standardisation does not explain the variation shown at GP practice level. • Over dispersion is shown when applying three standard deviations of the mean with between eight and 52 percent if practices lying outside these bounds • Further work is required to explore reasons for this variability. • possibly in emerging GP clusters, to explore practice variation, improve data quality and also help improve patient care. • Comparison with modelled data e.g. APHO diabetes population model • Findings are consistent with those found by Cardiff University in 2004-05.2 Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Conclusions from correlation between prevalence & deprivation • Many conditions demonstrate the expected association with deprivation, although this association is weak (but not all) • Calculation of practice deprivation scores may underestimate the correlation as practice catchment populations span areas of mixed deprivation levels • It can also highlight pockets of deprivation where a single practice may serve one specific area of deprivation in, an otherwise affluent area. • Student populations demonstrate deprived characteristics through the Townsend index. Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK
Epilogue – Data from Audit + • Audit + funded from GMS money • Data extraction is not free any new project needs to be funded • Data extraction needs approval from Audit + stake holders including GPC Wales new Information governance machinery to be satisfied • Data extraction should be of benefit to the general medical contractor Public Health Wales Observatory (PHWO) & Primary Care Quality & Information Service (PCQIS) – Martin.Holloway@Wales.NHS.UK