Download
1 / 31
310 likes | 372 Views
Prevention of preeclampsia. Jim Roberts. Introduction. The NICHD/NHLBI will soon begin a very large (9 to 12,000 women) and very expensive study of antioxidant therapy to attempt to prevent the pregnancy complication, preeclampsia. What background data and principles should guide such a study?.

E N D
Prevention of preeclampsia • Jim Roberts
Introduction • The NICHD/NHLBI will soon begin a very large (9 to 12,000 women) and very expensive study of antioxidant therapy to attempt to prevent the pregnancy complication, preeclampsia. • What background data and principles should guide such a study?
Goals • What is preeclampsia? • Prior attempts to prevent preeclampsia • What can we learn? • Principles to guide preventive therapy • Rationale for antioxidant therapy • Skeleton of study design (work in progress)
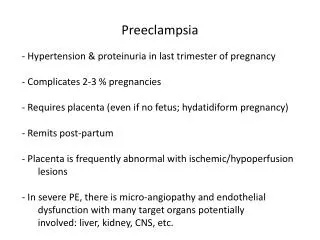
Preeclampsia • Clinical (pregnancy specific syndrome) • Hypertension • Proteinuria • Impact • Leading cause of maternal mortality • 5 fold increase in perinatal mortality • 15% of preterm births
Treatment of PreeclampsiaDelivery! • Usually prevents maternal mortality. • Does not prevent maternal morbidity. • Can result in iatrogenic prematurity.
Treatment of Preeclampsia • The best treatment is prevention!
Preeclampsia ProphylaxisHistory • Salt restriction • Salt supplementation • Protein restriction • Protein supplementation • Eat less • Eat more • Rest less • Rest more • etc., etc., etc. ...
Principles of Prophylaxis • Successful preventive therapy requires: • Sufficient understanding of the disease to direct strategy • The ability to identify patients at enough risk to justify prophylaxis • “Prophylactic” treatment may actually be early therapy. • Preventive therapy must prevent the disease and not merely the diagnosis of the disease.
“Decreasing the Diagnosis” • Preeclampsia is diagnosed by: • • increased blood pressure • • proteinuria • These are not important pathophysiological features! • Drugs which lower BP or prevents proteinuria will reduce the dx. • Have not prevented the disorder only the diagnosis.
Calcium SupplementationRationale • Hypocalcuria in preeclampsia • ? antedates disease • Increased intracytoplasmic calcium • platelets: • basal yes/no • stimulated yes/no • Epidemiology • low calcium diets => more preeclampsia • (South and Central America and Africa)
Calcium SupplementationClinical trials and meta-analysis OR for developing preeclampsia
Calcium SupplementationClinical trials and meta-analysis • Summary: • Preeclampsia reduced (OR = 0.38) • “PIH” reduced (OR = 0.3) • Blood pressure reduced (5.4 / 3.44) • “The minimal expense and negligible risk ... may justify administration of calcium to even the low risk cohort.”
Calcium SupplementationNIH trial • Design • • 4600 low risk nulliparous women • • Randomized to 2 gms Ca++ or placebo • • Assess calcium intake predelivery • • Assess urinary calcium in a subset
Why the Discrepancies?Calcium Trial Specific • Wrong amount of calcium? • • not likely • Compliance? • Poor definitions in the meta-analysis? • Supplement ≠ dietary calcium • Different populations? • • much more Ca++ deficient
Aspirin for PreeclampsiaRationale • “Prostacyclin thromboxane imbalance” • Prostacyclin • vasodilator inhibits platelet aggregation • made by endothelium • Thromboxane • vasoconstrictor aggregates platelets • made by platelets
Aspirin for PreeclampsiaRationale • “Prostacyclin thromboxane imbalance” • In preeclampsia the ratio of prostacyclin to thromboxane is reduced • (as predicted by the hypothesis) • But ... • These agents have very short half lives (i.e. they do not function as hormones)
Aspirin for PreeclampsiaRationale • “Prostacyclin thromboxane imbalance” • Aspirin given daily, in low doses, preferentially inhibits thromboxane synthesis.
Aspirin for PreeclampsiaClinical Trials • In the mid 1980’s several trials suggested benefit (less preeclampsia, reduced IUGR, fewer C-sections) in high risk patients. • Quality of trials varied (e.g. historical controls, non-blind etc.) • There were, however, several controlled trials suggesting benefits.
Aspirin for PreeclampsiaMeta-analysis • In 1991 metaanalysis of 6 highest quality studies (= 394)concluded that ASA: • 1. Reduced the incidence of preeclampsia • RR = 0.35 (0.22 - 0.55) • 2. Reduced the risk of IUGR • RR = 0.56 (0.36 - 0.88) • 3. Reduced the risk of C-section • RR = 0.34 (0.25 - 0.48)
Aspirin for PreeclampsiaLow Risk Studies *CLASP study patients are of "intermediate risk". 75% were entered because of a previous history of preeclampsia
Aspirin for PreeclampsiaCochranne Metanalysis • 35,000 women have taken ASA in RCT! • reduced preterm birth • reduced perinatal mortality • statisticaly but ? Clinically significant • Why so small an effect? • Subsets? • Wrong dose? • Wrong time in gestation? • Wrong time of day?
Why the Discrepancies?General metaanalysis vs. trial • GIGO (garbage in = garbage out) • Publication bias • • small negative trials do not get published (or submitted) • (at time of CLASP there were as many patients in unpublished studies as there were in the positive trials cited in the 1991 meta-analysis)
Why the Discrepancies?General meta-analysis vs. trial • Although the limitations of metaanalysis likely explain discrepancy, a caution is necessary. • • In large trials population is much less homogeneous than single center trials. • • Preeclampsia is heterogeneous. • • Perhaps only certain subsets benefit from a specific therapy.
What have we learned? • Meta-analysis is not a substitute for large clinical trials. • In testing preventive therapy for preeclampsia some marker of perinatal well being is the appropriate outcome. • It may be necessary to identify subsets of preeclamptic patients for effective early therapy.
Future DirectionsIdentifying targets for therapy • Preeclampsia: • • manifests many pathophysiological changes?cause or effect? • • is present before evident disease • • ends when pregnancy ends • • is likely the convergence of several pathways with a common endpoint
Future DirectionsIdentifying targets for therapy • Future trials should be guided by well established pathophysiological features. • • Biologically plausible antecedent of maternal/perinatal mortality/morbidity • • Present before disease • • Returns to normal after pregnancy • • May only be pertinent to a subset of preeclamptic women
Future DirectionsEffects on perinatal outcome • Signs of preeclampsia are not an important part of physiology. • As an inherited disease, predicts survival value of the disorder. • It is possible to mask the diagnosis without affecting relevant pathophysiology.
Future DirectionsEffects on perinatal outcome • Future clinical trials: • must be large enough to detect adverse fetal/neonatal outcome • should have as primary outcome an endpoint relevant to neonatal well-being
Future DirectionsEffects on perinatal outcome • Future clinical trials: • must be large enough to detect adverse fetal/neonatal outcome • should have as primary outcome an endpoint relevant to neonatal well-being • Admit our knowledge is limited and also collect mechanistic data (without compromising trial)