Download
1 / 53
680 likes | 1.84k Views
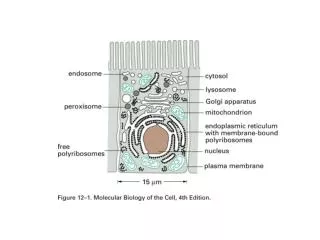
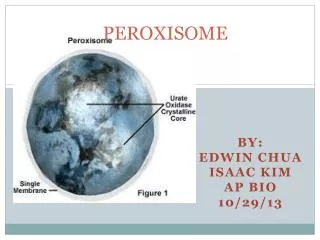
Disorders of Peroxisome Biogenesis (PBD). Nancy Braverman, M.S., M.D. McGill University-Montreal Children's Hospital Research Institute Montreal, QC. Spherical, single membrane bound, Diameter = 0.2 - 1 µm, several hundred/cell All eukaryotes. Properties of peroxisomes.

E N D
Disorders of Peroxisome Biogenesis (PBD) Nancy Braverman, M.S., M.D. McGill University-Montreal Children's Hospital Research InstituteMontreal, QC
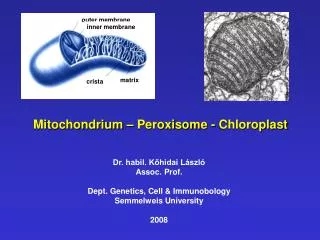
Spherical, single membrane bound, Diameter = 0.2 - 1 µm, several hundred/cell All eukaryotes Properties of peroxisomes
Timeline of discovery 1958:Peroxisomes 1st described 1964:Zellweger cerebro-hepato-renal syndrome 1973:Abnormal peroxisomes in ZS 1983:PBD, a paradigm for metabolic malformation syndromes 1987:Complementation groups reflect genetic heterogeneity in PBD 1990:Peroxisome biogenesis (PEX) genes identified in yeast 1994:Human genes identified by yeast homology >2000:Study of protein functions, pathophysiology, applications to management and therapy
Organelles • Benefits • concentrate enzymes and substrates • sequester toxic substances • Requirements • targeting systems • transporters, receptors • Consequences • genetic diseases ofthe components Nucleus Px Mt ER
Peroxisome assembly (PEX) genes • Encode proteins (peroxins) required for matrix protein import, peroxisome division and membrane formation • 14 human PEX genes; 13 thus far responsible for PBD • 26 different PEX genes among eucaryotes
Peroxisomes originate from ER membranes and by fission of existing peroxisomes NEXT >> Click to view animation >> adapted from Annu Rev Genet. 2000;34:623-652. Sacksteder KA, Gould SJ.
Role of peroxins in matrix protein import Click to view animation >> Gould, Raymond, Valle.In: Metab & Molec Basis of Inh Dis. Ch 129 p. 3190.
Enzymatic pathways in peroxisomes • Fatty acid oxidation (VLCFA, PA) • H2O2 detoxification (catalase) • Docohexanoic acid (DHA) synthesis • Bile acid synthesis • Plasmalogen (ether phospholipid) synthesis • Cholesterol synthesis • Glyoxylate detoxification • Lysine catabolism (pipecolic acid)
Contain Peroxisome Targeting Sequences (PTS) Imported as oligomers/fully assembled proteins Can have dual localizations in mitochondria, cytosol Properties of peroxisomal matrix proteins PTS1 PTS2 -SKL R/KLX5Q/HL -SKL N - terminal (-R/KLX5 Q/HL-) Presequence cleaved internally 3 enzymes only: Thiolase, PhyH, AGPS Receptor is PEX7 C - terminal (-SKL) Most matrix proteins Receptor is PEX5
Peroxisomal β-Oxidation Click to view animation >>
α- oxidation and auxillary enzymes in β-oxidation Click to view animation >>
Synthesis of docohexanoic acid (DHA) requires peroxisomal β-oxidation Click to view animation >> J. Biol Chem. 2001; 276:38115-20. Su HM, Moser AB, Moser HW, Watkins PA
Plasmalogen lipids Plasmalogens are glycerol-based phospholipids with a vinyl ether-linked alkyl group in the C-1 position Vinyl ether-linked alkyl chain at C-1 • Plasmalogens are abundant in nervous tissue and erythrocyte membranes as • phosphatidyl-choline • phosphatidyl-ethanolamine CH2-O-CH=CH-R O CH-O-C-CH2-R2 CH2-OPO3-ethanolamine or -choline • Functions: • antioxidant • DHA storage • lipid messengers (PAF) • vesicle formation Plasmalogen
Plasmalogen biosynthesis is initiated in peroxisomes Click to view animation >>
Genetic disorders of peroxisomes • Multiple enzyme deficiencies: Peroxisomal Biogenesis Disorders (PBD) • Zellweger spectrum disorder (ZSD) (~1/60,000) • Rhizomelic chondrodysplasia punctata spectrum (RCDP)(~1/100,000) • Single enzyme deficiencies • X-linked adrenoleukodystrophy (X-ALD) (~1/20,000) • 3-methyl-CoA racemase deficiency • Adult Refsum disease • Hyperoxaluria Type I
Some single enzyme deficiencies can mimic PBDs • VLCFA oxidation → Zellweger spectrum disorder • Acyl-CoA oxidase • D-Bifunctional protein (hydratase/dehydrogenase) • Plasmalogen biosynthesis → RCDP spectrum • DHAPAT (RCDP2) • ADHAPS (RCDP3) • Some PBDs mimic SEDs → • Adult Refsum disease causes PEX7 deficiency
Zellweger spectrum disorder (ZSD), a clinical continuum Zellweger Syndrome Infantile Refsum Disease
Craniofacial dysmorphism (ZS) • Widely patent fontanels and sutures • Prominent high forehead • Shallow orbital ridges • Low broad nasal bridge • Anteverted nares • Hypertelorism • Epicanthal folds • High arched palate • Micrognathia • Redundant skin folds of neck
Neuronal migration defects (ZS): Polymicrogyria, pachygyria, heterotopias
Neonatal adrenoleukodystrophy • 15 mo old with FTT • Weight: 50th% for 6-mo old • Height: 10th% • Frontal bossing • Wide anterior fontanel • Depressed nasal bridge • Epicanthal folds • Diffuse hypotonia • White matter changes on MRI • Developmental delays and seizure disorder
Infantile Refsum disease? • 42-yr old woman • Hearing loss at 2-3 yrs • Progressive retinal disease • Legally blind at 11 yrs • Intermittent behavioral/psychiatric problems • Lives in a group home
Disease course • About 1/2 of PBD patients have NALD-IRD phenotypes • Patients show progressive deterioration over time and become blind, deaf and loose cognitive abilities • Deterioration may coincide with onset or progression of leukodystrophy • If effective treatment was available, it might halt the disease progression
Infantile Refsum disease • Diagnosed ~18 months • RP and hearing loss • Walked at ~30 months • Developed seizures at 4 yrs • Deterioration in vision • Moderate to severe MR
Rhizomelic Chondrodysplasia Punctata (RCDP) Dysmorphicfacies: frontal bossing, short saddle nose with antevertednares, congenital cataracts profound impairment of growth and mental retardation, variable survival
Skeletal changes in RCDP • Rhizomelia, metaphyseal flaring • Epiphyseal stippling, small thorax • Vertebral coronal clefts • Mineralization of intervertebral discs, contractures
Clinical spectrum of RCDP • 6-yr old: moderate MR, cataracts and CDP, but no rhizomelia or growth failure • 20-yr old, congenital cataracts, mild learning disability, normal stature, no rhizomelia, no CDP • 66-yr old initially diagnosed at 7-yrs with adult RD
Confirmation of metabolite testing • Establish a fibroblast culture for • VLCFA content • Plasmalogen synthesis • Phytanic acid oxidation • Catalase solubility • Immunocytochemistry • DNA testing
ZSD: Challenges to Diagnosis • Patients with mild or atypical clinical presentation • Patients with mild or atypical biochemical profile • Patients with biochemical abnormalities in blood, but normal studies in fibroblasts (peroxisomal ‘mosaicism’) • Patients with abnormal peroxisome morphology and soluble catalase in hepatocytes, but normal studies in fibroblasts (peroxisomal ‘mosaicism’) • Patients with abnormal peroxisome morphology and soluble catalase in some cells, adjacent to other cells that are normal in liver and fibroblasts (peroxisomal ‘mosaicism’)
Mosaic pattern of peroxisome matrix proteins in liver biopsy specimen from an IRD patient Immuno-gold staining for alanine-glyoxylate aminotransferase is granular when the enzyme is inside the peroxisome Credit to Frank Roels
Mosaic pattern of peroxisome matrix proteins in cultured fibroblasts from PBD patients Credit to N. Braverman
In ZSD, phenotype correlates with severity of protein import defect, peroxisome number and size PX # and size Matrix protein import Control ZS IRD
ZSD: Approaches to Mutation Identification • 1. Complementation by somatic cell hybridization • 2. Complementation by transfection of PEX cDNAs • 3. Targeted sequence analysis of specific PEX genes Hierarchal algorithm based on common mutations and frequency of each PEX gene defect Molecular analysis is used for carrier detection, prenatal diagnosis, preimplantation genetic diagnosis, prognostic value, difficult cases • 4. Next generation sequencing platforms
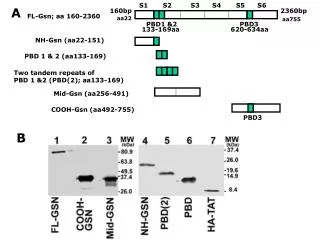
Mutation analysis of PEX genes • 2 mutations in PEX1 account for 56% of ZSD • PEX6, 26, 10, 12 account for 26% of ZSD • 2 mutations in PEX7 account for 65% RCDP • Association of severe mutations with severe disease
In ZSD, phenotype does not correlate to specific PEX gene defects
Role of peroxins in matrix protein import Click to view animation >> Gould, Raymond, Valle.In: Metab & Molec Basis of Inh Dis. Ch 129 p. 3190.
Contrast ZS and RCDP • ZS • both PTS1 and PTS2 defects • reduced number and size of peroxisomes • RCDP • PTS2 defect only (PTS1 normal) • peroxisomal morphology normal • RCDP should represent a segment of ZS, but there are more severe abnormalities of bone, lens, different CNS defects and skin
Tools: mouse models, mammalian cell culture, pathology investigations, other model organisms • Neuron migration and integrity • Accumulation of reactive oxygen species • Role of mitochondria in peroxisome disorders • Accumulation of VLCFA and BCFA • Deficiency of ether phospholipids • Peroxisomes functions in development and differences between tissues/organs Pathogenesis of PBD
Peroxisome single enzyme defects: X-linked Adrenoleukodystrophy
X-linked adrenoleukodystrophy (X-ALD) • Medical history • 8-year old previously healthy, typically developed male • Attention deficit/hyperactivity apparent within the past year • Performing poorly in 2nd grade • Recently began to run clumsily and to walk stiffly • No recent illnesses • No medications
X-ALD Deterioration in writing over a 4 month period Brain MRI – white matter disease Dec 29, 1989 Mar 5, 1990 May 3, 1990
X-ALD • Defect in peroxisomal very long chain fatty acid oxidation • Adrenoleukodystrophy protein (ALDP) gene (ABCD1) • Mapped to Xq28 • Over 200 mutations known, most crm negative • Incidence ~ 1/20,000 • All ethnic groups
X-ALD: defective peroxisomal β-oxidation Click to view animation >>
ALD protein Homology with ABC half-transporter family No homology with fatty acyl-CoA synthetases Yet, the biochemical defect is in the activation of very long chain fatty acids to acyl-CoA esters in peroxisomes VLCFA + CoA + ATP VLCFA-CoA Exact mechanistic link between ALDP deficiency and VLCFA activation is yet undefined May be defective transport of VLCFA across peroxisomal membrane
Childhood cerebral form ~35% Onset - ~6-12 yrs (survival: several years) 90% with adrenal insufficiency Adrenomyeloneuropathy (AMN) ~50% Spastic paraparesis and sphincter dysfunction Onset - ~2nd-5th decade (survival: decades) 2/3 with adrenal insufficiency Other phenotypes ~15% Addison disease only Adult-onset cerebral involvement - dementia Female heterozygotes- 50% with mild AMN-like Sx Multiple phenotypes of X-ALD
X-ALD laboratory evaluation • Plasma VLCFA analysis • Elevated C26:0 and C24:0 • Elevated C26:0/C22:0 and C24:0/C22:0 ratios • Mutation analysis (ABCD1 gene) useful for heterozygote detection
Resolution of lyso-PC’s during LC-MS/MS analysis Newborn screening for X-ALD: pilot project stage (Hubbard et al, 2007) • Collision assisted decomposition of lyso-PCs results in fragmentation LC–MS/MS data from NB blood spots for 26:lyso-PC
X-ALD treatment • Dietary therapy • Restriction of dietary VLCFA intake • Lorenzo’s oil- 4:1 mix • Glycerol trioleate (C18:1) • Glycerol trierucate (C22:1) • Lowers plasma C26:0 and C24:0 levels