Download
1 / 53
530 likes | 560 Views
Learn about Staphylococcus, its classification into coagulase-positive and coagulase-negative subgroups, and its pathophysiology including bacterial virulence factors such as toxins, enzymes, and modes of infection.

E N D
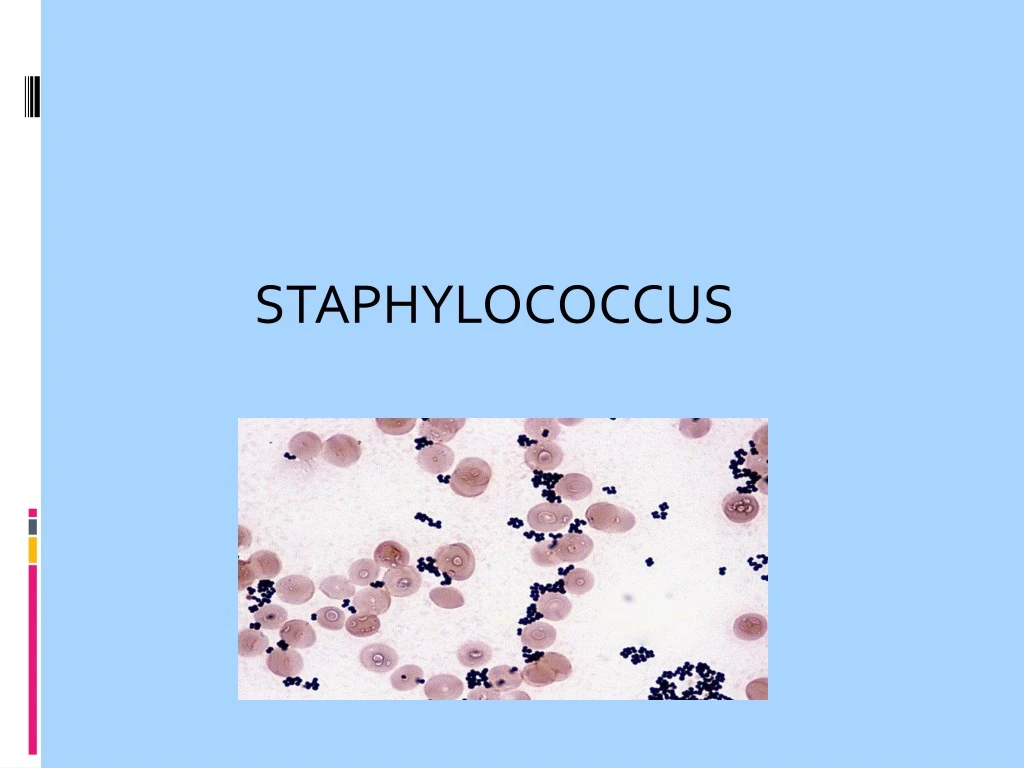
Introduction • Sir Alexander Ogston, a Scottish surgeon, first showed in 1880 that a number of human pyogenic diseases were associated with a cluster-forming micro-organism. • He introduced the name 'staphylococcus' (Greek: staphyle = bunch of grapes; kokkos = grain or berry),
Cluster formation is due to cell division in 3 planes with daughter cells remaining close to one another
Classification • Family : Micrococcaceae • Genus: Micrococcus and Staphylococcus •The genus Staphylococcus can be divided into two subgroups (on the basis of its ability to clot blood plasma by enzyme coagulase): • coagulase-positive • coagulase-negative.
Species: The genus Staphylococcus contains about forty species and subspecies today. Only some of them are important as human pathogens: –Staphylococcus aureus –Staphylococcus epidermidis –Staphylococcus hominis –Staphylococcus haemolyticus –Staphylococcus saprophyticus –others
Pathophysiology Bacterial Virulence Factors :- S.aureus expresses a variety of virulence factors on its surface and also produces a large number of toxins & enzymes which collectively help it to cause infection & disease. Virulence factors may be -> A. Cellular (Cell wall associated) B. Extra-cellular virulence factors
Cellular virulence factors Capsule -> capsular polysaccharide present as outermost layer in some strains, has potent antiphagocytic action Peptidoglycan -> • has endotoxin like action; • activates complement; • stimulates IL-1 production from macrophages; • chemotactic for PMNLS
Teichoic acids -> • Polymers of glycerol / ribitol phosphate, bound to peptidoglycan • Help in adherence to host cells • Has anticomplementary activity Protein A -> • Present on cell surface & helps in adherence • Chemotactic for PMNLS • Has antiphagocytic activity • Has anticomplementary activity
Clumping factor -> • Also known as “bound coagulase” • Is responsible for clumping of S.aureus cells in a suspension when mixed with human / rabbit plasma • Act by forming a fibrin clot around the bacterial cells
Extra-cellular virulence factors Toxins -> A. Hemolysins • Alpha (α) toxin – hemolytic; leucocidal; cytotoxic; dermonecrotic & lethal • Beta (β) toxin – a hemolytic sphingomyelinase • Gamma (γ) toxin – hemolytic • Delta (δ) toxin – disrupts biological membranes & is hemolytic
B. Leucocidin -> - Cytotoxic to leucocytes - Also known as the “Panton – Valentine” (P-V) leucocidin - An important virulence factor of ‘Community acquired methicillin resistant S.aureus’ (CA-MRSA)
C. Exfoliative (Epidermolytic) toxins) -> - Two types – ‘A’ & ‘B’ - Responsible for generalized desquamation seen in “staphylococcal scalded skin syndrome” - Also act as ‘superantigens’
D. Enterotoxins -> - These are multiple toxins responsible for ‘toxic type of food poisoning’ - Types are –> A – E; G – J; K – R ; U and V - At least 5% of S.aureus produce one or more of these toxins. - Cause vomiting & diarrhea within 8 hrs of ingestion of toxin. - Emetic effect is due to stimulation of ‘vomiting centre’ in CNS after toxin binds to neural receptors in the GIT
E. Toxic Shock Syndrome Toxin – 1(TSST-1) -> - 5– 25% isolates of S.aureus produce this toxin. - Responsible for the condition – “Toxic shock syndrome” - A super antigen which activates a large no. of T cells, thereby stimulating release of large amounts of inflammatory cytokines which cause damage to host.
- Cytokine activity leads to damage to several organs, fever, shock & desquamation of skin
2. Enzymes Coagulase –> an enzyme produced by S. aureus which has the ability to convert fibrinogen to fibrin clot. Two types – > Free coagulase – detected by the ‘Tube coagulase test’ and > Bound coagulase (clumping factor) – detected by the ‘Slide coagulase test’
Other enzymes of S.aureus Several other enzymes are also produced by S.aureus, which help the organism in its pathogenesis. . Hyaluronidase . Lipase . Staphylokinase . Beta-lactamases . Nucleases
Pathogenesis Source of Infection -> Patients – who are suffering from pyogenic infections such as boils, pustules, carbuncles, infected wounds. Carriers- healthy individuals who usually harbour S.aureus in the anterior nares (nasal carriers) - Approx. 10-30 % of a normal population will be carriers of S.aureus
Mode of infection -> Direct contact or indirect contact (fomites) with the infective exudates. Clinical findings -> Clinical manifestations caused by S.aureus can be divided into two categories – - Pyogenic infections - Toxin mediated diseases
Pyogenic infections Superficial infections -> • Folliculitis • Boils • Furuncles • Carbuncles • Impetigo • Mastitis • Abscesses • Cellulitis • Wound / Surgical wound infections • Involved in development of – acne, eczema, pyoderma
Deep infections -> These are not commonly seen in healthy individuals but in persons with :– - defective phagocytosis - Immunosuppression - Diabetes - After trauma
Entry of S.aureus into blood stream results in the organism being seeded into several organs causing :- Septicemia Endocarditis Osteomyelitis Meningitis Empyema Pneumonia Chronic focal suppuration of any organ
Staphylococcal toxin mediated diseases Due to the effect of toxins produced by S.aureus on the target tissue / organs. Food poisoning (Gastroenteritis) -> Toxic type, due to ingestion of preformed toxin in protein/carbohydrate rich food, causing vomiting & diarrhea. Features – Short incubation period (1 – 8 hrs) Fever is absent Self limited Food items involved – milk products, fish, meat
Skin exfoliative diseases -> - Bullous impetigo - Pemphigusneonatorum - Scalded skin syndrome (SSS) Usually seen in children and is due to the production of exfoliative toxins. Characterized by fever, large bullae, erythematous macular rash, with large areas of skin being sloughed off, serous fluid exudation; hair & nails may be lost. Recovery occurs by 7-10days.
Toxic shock syndrome ->Due to Toxic shock syndrome toxin (TSST) A multisystem disease with symptoms such as . Fever, Myalgia . Hypotension . Vomiting, Diarrhoea . Rash, Desquamation . Cardiac and Renal failure in severe cases. - Seen in young women using tampons during menstruation and in children and men with staphylococcal wound infection
Lab diagnosis Specimen collected -> Sampling depends on type & localization of infection. - Surface swabs - Pus - Blood - Aspirates - Sputum - CSF
Methods:- Microscopy -> Gram’s stained smear – will show gram positive cocci in clusters along with pus cells.
Culture methods -> Media used :- - Basal medium -> Nutrient agar - Enriched media -> Blood agar, Chocolate agar - Selective medium -> Mannitol salt agar - Media are inoculated with specimen and incubated at 37OC for 24-48hrs.
Identification of isolates as S.aureus -> 1. Golden yellow colonies (not always) 2. Beta hemolysis around colonies on blood agar
3. Gram’s smear of growth -> gram positive cocci in clusters 4. Catalase test -> Positive 5. Coagulase test -> Positive 6. Mannitol fermentation -> Positive
3. Antibiotic susceptibility testing -> Susceptibility testing has to be carried out on all isolates of S.aureus as they demonstrate high level of resistance to several antibiotics. 4. Typing methods -> required for epidemiological purposes • Antibiogram typing • Phage typing • Pulsed-field gel electrophoresis typing • Multi-locus sequence typing
Treatment • Wounds, abscesses, etc. must be cleared of pus & necrotized tissue. • Topical application of antibiotics such as Mupirocin. • For penicillin resistant strains, - Oxacillin/Cloxacillin/Methicillin/Nafcillin or combination of Amoxycillin/Clavulinicacid. • For MRSA strains, - Vancomycin is the drug of choice
For eradication of carrier status –> - intranasal application of mupirocin, - Oral rifampin
Control measures In hospitals -> • Carrier status of hospital personnel should be determined and such individuals treated • NICU, ICU and OT’s should be out of bounds to carriers. • Routine hand-washing should be strictly followed by health care personnel in between patients. • Cleanliness, hygiene & aseptic management of lesions
Coagulase-negative staphylococcal spp (Cons)
Coagulase-negative staphylococcal spp (Cons) Colonizes moist body areas such as axilla, inguinal and perianal areas, anterior nares and toe webs. Important cause of nosocomial infection esp. S. epidermidis. Usually causes nosocomial infections in patients with predisposing factors such as immunodeficiency/ immunocompromised or presence of foreign bodies
Staphylococcus epidermidis Is part of the normal skin flora but can cause opportunistic infections in conditions such as: . IV catheters . Prosthetic implants (heart valves, vascular grafts, joints) . Peritoneal dialysis patients with indwelling catheters . CSF shunts . UTI in catheterized patients
Virulence factor:- Production of large amounts of glycocalyx which help in adherence & micro colony formation. Such strains are highly resistant to most antibiotics.
Staphylococcus saprophyticus • Importance of S.saprophyticus. • S. saprophyticus frequently isolated in rectum and genitourinary tract of young women. • Can be causative agent in UTI in young healthy women. • 2nd most common urinary pathogen (other than E. coli) in uncomplicated cystitis in young women.
What Is MRSA? MRSA is the term used for any strain of Staphylococcus aureus that has developed resistance to β- lactam antibiotics, which include the penicillins (methicillins, oxacillin, dicloxacillin etc.) and cephalosporins. MRSA causes a variety of disseminated, lethal infections in humans. Has the ability to easily transfer resistant genes to other species directly and indirectly.
How MRSA is resistant to methicillin • MRSA can be due to 3different resistance mechanisms – Production of penicillin-binding protein 2a (PBP2a) encoded by mecA gene. – Production of beta-lactamase. – Production of modified intrinsic PBPs.
Detection of MRSA • Resistance due to mecA can be detected via cefoxitin disk diffusion or dilution methods according to CLSI breakpoints. • Resistance due to beta-lactamase production can be detected via the use of beta-lactamase inhibitor such as clavulanic acid (disk diffusion method) which would result in an increase in zone size or decrease of 2dilutions.
How is MRSA spread Direct contact with infected or colonized host -human-to-human contact. Contaminated intermediate surfaces -hand towels faucets -tub/shower. Airborne fluid droplets.
CA-MRSA and HA-MRSA • CA-MRSA Unique microbiologic and genetic properties compared with HA-MRSA. • May allow the community strains to spread more easily or cause more skin disease • CA-MRSA skin infections are known to spread in crowded settings
HA-MRSA Healthcare-acquired Methicillin resistant Staph. aureus • Lead to redness, swelling and pain resembling to spider bite. • Minor skin problems pimples, insect bites, cuts, and scrapes especially in children may lead to MRSA colonization.
Vancomycin resistance • Isolate of S. aureus in 1997was observed resistant by an unusually thickened cell wall containing dipeptides. Thereby reducing availability of the drug for intracellular target molecules. This was the first observation of vancomycin intermediate S. aureus (VISA).
The first description of vancomycin-resistant S. aureus (VRSA). was observed for the first time in 2002; • The predicted mechanism of van A gene plasmid-mediated transfer from enterococci to S. aureus.