Download
1 / 24
240 likes | 390 Views
First Steps in Response to a Radiological Terrorist Incident. Dale Dusenbury,CHP North Carolina Division of Radiation Protection.

E N D
First Steps in Response to a Radiological Terrorist Incident Dale Dusenbury,CHP North Carolina Division of Radiation Protection
“Protecting America's homeland and citizens from the threat of weapons of mass destruction is one of our Nation's important national security challenges... prudence dictates that the United States be fully prepared to deal effectively with the consequences of such a weapon being used here on our soil. “ President George W. Bush May 8,2001
Assumptions • Success for the terrorist consists of creating fear and disruption, no matter the damage done or the lives lost. • Firefighters, police, and public safety are expected to encounter the incident initially. • If state health physics specialists are available, they will also be tasked to respond to an incident of nuclear terrorism.
What We’re Doing • The Division of Radiation is supplementing existing capabilities in three areas: • Applying Guidance • Procedure Revisions • Dose Projection Capability
Health Physics Guidance • The NCRP has provided Report 138 to provide guidance in areas of: • Definition of Phases • Medical Management • Psychosocial Effects. • Command and Control • Public Communication • Dose Limitation
Phases of Terrorist Incident • Early Phase-Begins with start of incident and continues while material is released. • Intermediate Phase-Begins when release has ended, cloud of contamination has settled, and rescue efforts have been terminated. • Late Phase-material has been incorporated into environment and sampling results are available. Ends when restrictions lifted.
Early Phase:Defining the Incident • Two dose rate levels used by first responders: • 10 mrem/hr(0.1 msV/hr) for Control area • 10 rem/hr(0.1 Sv/hr) for Turnback area. • Evacuate or shelter areas downwind, set up control area. Set up monitoring/decon stations. • Dose projection should be performed for the communities downwind
Intermediate and Late Phase Activities • Environmental radiation measurements needed to define the contamination zone. • Carry out evacuation and food interdiction actions to prevent public exposure. • Assemble a plan to conduct further surveys and environmental sampling. • Model deposition via AMS data & in-situ measurements. • Set up Assessment Center
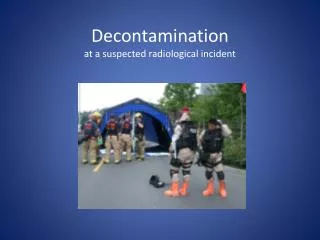
Medical Management • First, of all stabilize those with life threatening injuries. • Use standard triage to assign priority to those with other injuries. • Separate contaminated from non-contaminated patients, allowing for preliminary decon. • Patients with wounds require special care.Clothing and excreta should be collected.
Radiological Assessment and Decon • Use detector sensitive to alpha,beta, and gamma i.e. Thin window GM. • Map contamination on body. • Remove clothes and store for disposal. • Decon using tepid water, w/ or w/o detergent. • Remove hair by cutting. Amputation not recommended to remove contamination.
Psychosocial Effects • Without considering psychosocial effects, your response can be technically “correct”, yet people will still get sick and mistrust you. • Examples: Chronic stress, with or w/o exposure Survivor Guilt Mental Health Problems & PTSD Stigma(Goinea Residents)
Prevention • Plan to deal with these issues as part of exercises, etc. • Openness in decision making is required, so identify stakeholders if possible.
Command and Control • States often use an ICS (incident command system) to respond. • Although the states keep public health responsibilities, a terrorist incident requires federal response. • The Attorney General has been given responsibility to lead such a response through the FBI.
Public Communications • Goal:Achieve trust and credibility. • State, Federal, Local governments need to establish communications plans before an event. • Coordinated information release is to be done by JIC, which can adapt to long term needs. • An Internet template for JIC should be set up and exercised.
Dose Limitation Concepts • Philosophy(based on ICRP system): • Prevent occurrence of deterministic effects due to radiation exposure. • Limit stochastic effects, such as cancer and genetic effects to reasonable levels.
Dose Limitation Concepts • Philosophy(based on ICRP system): • When 5 Rem/yr(50 mSv/yr) for workers of 100 mrem/yr(1 msV/yr) for public exposure may be exceeded a different concept is required. • Dose reductions should outweigh disadvantages of intervention actions.
Emergency Worker Guidance • Exposures should be kept less than the occupational limits when lifesaving/rescue is not involved. • Where it is not possible to carry out the above, ICRP recommendations(1991) are: • 50 Rem(0.5 Sv) effective dose • 500 Rem(5 Sv) equivalent dose to skin • Knowledgeable volunteers should be used.
Protecting Emergency Workers • Two limits: Control Area Limit: 10 mrem/hr(0.1 mSv/hr) to define exclusion area. Turnback Level-10 rem/hr(0.1 Sv/hr) and 10 rem(0.1 Sv) total dose. Allows for work inside the zone.
NCRP 138-Recommendations • General Public Countermeasures(Effective dose) Sheltering: 0.5-5 Rem(5-50 mSv) Evacuations:5-50 Rem(50-500 mSv) KI(special populations):5 Rem-50 Rem(50-500mSv) Relocation:1 Rem/month(10 mSv/month) or 100 Rem(1000mSv) total
NCRP 138-Recommendations • Recovery Workers Countermeasures(Effective dose) Annual Limit: 5 rem/yr(50 mSv/yr) • Recovery Workers(Emergency Actions) 50 rem(500 mSv). • Single Foods: 1 rem/yr(10 mSv/yr).
Procedure Evaluation • Currently reviewing procedures incorporating response to nuclear weapons accidents used to support FRMAC. Example: DOD 51 00.52-M Radiological Hazard and Safety Environmental Monitoring
Tools: The HOTSPOT Codes • Designed for short term events(< 24 hours) • Uses Gaussian Plume model for dose projection. Uses editable library. • Does not calculate shine doses from elevated plume. • Calculates effective doses. • Models fire, explosion, tritium release, weapons detonation.
References • www.llnl.gov/nai/technologies/hotspot/ • http://web7.whs.osd.mil/text/p31508m.txt