Download
1 / 9
90 likes | 106 Views
Explore the MARCH Study on switching to MVC in HIV treatment, focusing on virologic outcomes, safety, and treatment efficacy over a 48-week period. Findings suggest MVC is a viable switch option for patients on specific regimens.

E N D
Switch to MVC • MARCH Study
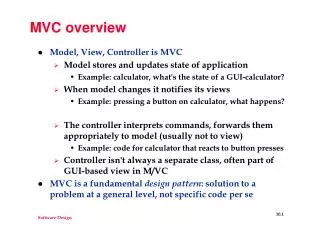
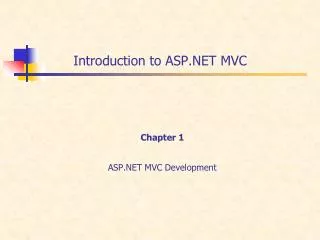
MARCH Study: switch to MVC • Design Randomisation 1 : 2 : 2 Open-label W48 W96 Adults ≥ 18 years Stable (> 24 weeks) 2 NRTI + PI/r regimen HIV RNA < 200 c/mL CCR5 virus on proviral DNA tropism testing No previous virological failure No resistance to study medications HBs Ag negative N = 82 Continuation of 2 NRTI + PI/r 2 NRTI + MVC 300 mg BID N = 156 PI/r + MVC 150 mg BID N = 157 • Objective • Primary Endpoint: proportion with HIV RNA < 200 copies/mL at W48 • Non inferiority of the switch arms vs control, by intention-to-treat, lower margin of the two-sided 95% CI for the difference = - 12 %, 80 % power Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
MARCH Study: switch to MVC Baseline characteristics and disposition Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
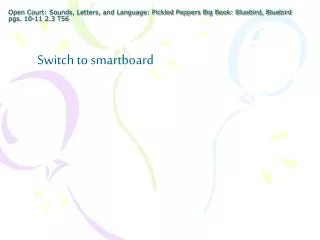
MARCH Study: switch to MVC Virologic Outcomes – W48 Intention to Treat Analysis 2 NRTI + PI/r 2 NRTI + MVC PI/r + MVC % 97.6 100 95.1 93.6 * 91.7 84.1 ** 77.7 80 60 40 20 0 HIV RNA < 50 c/mL HIV RNA < 200 c/mL (primary endpoint) * ≠ : - 4% ; (95% CI = - 9.0 to 2.2) ** ≠ : - 13.5% ; (95% CI = - 19.8 to -5.8) Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
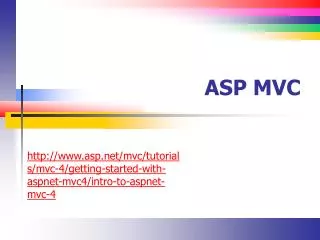
MARCH Study: switch to MVC % with virologic response (HIV RNA < 200 c/mL), by week 1.00 0.75 2 NRTI + PI/r 2 NRTI + MVC PI/r + MVC 0.50 0.25 Hazard ratio for loss of virological response < 200 c/mL over 48 weeks: 2.41 (95% CI: 1.31-4.43 ; p = 0.005) for the MVC + PI/r arm vs control arm 0.00 0 12 24 36 48 60 72 84 96 Week Number at risk 2 NRTI + PI/r 2 NRTI + MVC PI/r + MVC 82 156 157 81 149 151 80 143 137 80 139 134 77 132 123 59 103 98 45 90 65 36 86 54 17 60 36 Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
MARCH Study: switch to MVC Emergent resistance in participants with confirmed virologic failure Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
MARCH Study: switch to MVC Changes in immunologic and metabolic parameters and quality of life over 48 weeks p: vs 2 NRTI + PI/r Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
MARCH Study: switch to MVC Safety at W48 One myocardial infarction was reported on MVC in a patient with increased CVD risk due to lifestyle and cardiac congenital malformation Pett SL. Clin Infect Dis 2016;63:122-32 MARCH
MARCH Study: switch to MVC • Conclusion • This large international randomised study demonstrates that MVC with a 2-N(t)RTI backbone, in those with R5-tropic virus determined by genotypic tropism testing, is a switch/simplification option for patients virologicaly suppressed on PI/r + N(t)RTI regimens • MVC was safe and well tolerated, with favorable impact on lipids and neutral effects on renal function over 48 weeks • These data support MVC as a switch option for ritonavir-boosted PIs when partnered with a 2-N(t)RTI backbone, but not as part of N(t)RTI-sparing regimens comprising MVC with PI/r Pett SL. Clin Infect Dis 2016;63:122-32 MARCH