Download
1 / 30
360 likes | 1.29k Views
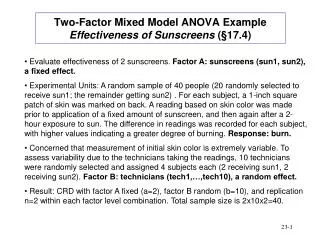
SUNSCREENS. Skin damage from radiation is cumulative whether sunburn occurs or not. Annual incidence: 500,000 cases of basal cell CA occur. 100,000 cases of squamous cell CA occur. 20,000 cases of malignant melanoma occur. ULTRAVIOLET RADIATION SPECTRUM. UVA (Longwave Radiation)

E N D
SUNSCREENS Skin damage from radiation is cumulative whether sunburn occurs or not. Annual incidence: • 500,000 cases of basal cell CA occur. • 100,000 cases of squamous cell CA occur. • 20,000 cases of malignant melanoma occur.
ULTRAVIOLET RADIATION SPECTRUM UVA (Longwave Radiation) • Range 320-400 nm • Erythrogenic activity is weak, however penetrates dermis • Responsible for development of slow natural tan • Most drug-induced photosensitivity rxn occurs • UVA may augment the effects of UVB
ULTRAVIOLET RADIATION SPECTRUM UVB (Middlewave Radiation) • Range 290-320 nm • Erythrogenic activity is the highest • Produces new pigment formation, sunburn, Vit D synthesis • Responsible for inducing skin cancer
ULTRAVIOLET RADIATION SPECTRUM UVC (Shortwave or Germicidal Radiation) • Range 100-290 nm. • Does not reach the surface of the earth. • Is emitted from artificial ultraviolet sources.
ULTRAVIOLET RADIATION SPECTRUM • Long-term hazards of skin damage from radiation: • Malignancy: • Squamous cell epithelioma • Actinic keratosis • Basal cell carcinoma • Premature aging • nevus, seborrheic keratosis, solar lentigo • wrinkles, lines, etc
SUNSCREEN CLASSIFICATIONS • Physical • Opaque formulations containing: • titanium dioxide • talc, kaolin • zinc oxide • ferric chloride • icthyol, red petrolatum • Mechanism: scatters or reflects UV radiation due to large particle size
SUNSCREEN CLASSIFICATIONS • Chemical • Formulations containing one or more: • PABA, PABA esters • benzophenones • cinnamates • salicylates • digalloyl trioleate • anthranilates • Mechanism: absorbs UV radiation
SUNSCREENS • Sun Protection Factor (SPF) = MED of Photoprotected Skin MED of Unprotected Skin • MED is minimum dose of radiation which produces erythema • SPFs are determined indoors using xenon lamps which approximate the spectral quality of UV radiation
SUNSCREENS • Factors which influence effectiveness of SPFs • Difference in skin types. • Thickness of the applied sunscreen. • Time of day. • Altitude: each 1,000 ft increase adds 4% to the intensity of erythema producing UV radiation; thus intensity is about 20% greater in Pocatello than at sea level. • Environment: snow/white surfaces reflect 70-90%, and when directly overhead water reflects nearly 100% of UVR. • Vehicle: determines skin penetration of sunscreen.
SUNCREEN AGENTS PABA (Para-aminobenzoic acid) • Very effective in the UVB range(200-320 nm). • Most effective in conc of 5% in 70% ethanol. • Maximum benefit when applied 60 min prior to exposure (to ensure penetration and binding to stratum corneum). • Does NOTpreventdrug/chemical-induced photosensitivity rxn. • Contact dermatitis can develop. • May produce transient drying/stinging from alcohol content (may be alleviated by adding 10-20% glycerol). • May stain clothing.
SUNCREEN AGENTS PABA Esters (Padimate A, Padimate O, Glyceryl PABA) • Also very effective in UVB range (280-320) • Most effective in conc. 2.5-8% in 65% alcohol • May penetrate less effectively than PABA • Similar application and adverse effect • Less staining
SUNCREEN AGENTS Benzophenones (oxybenzone, dioxybenzone, sulisobensone) • Slightly less effective than PABA. • Absorbs from 250-400 nm spectrum (ie, UVA & UVB). • Combinedwith PABA or PABA ester improves penetration and is superior to either agent used alone (200-400 nm wavelength coverage). • Beneficial in preventing photosensitivityrxns. • Contact dermatitis is rare.
SUNCREEN AGENTS Cinnamates and Salicylates • Minimally effective, absorb UVB spectrum. • Generally used in combination with one of the above.
SUNCREEN AGENTS Anthranilates • Minimally effective, absorbs UVA spectrum 250-322 nm. • Usually combined with UVB agent to broaden spectrum.
USE IN YOUNG CHILDREN • Not recommended in children < 6 mos (due to theoretical concern that percutaneous absorption may be greater and excretory functions may not be mature enough to handle). • No reported cases of toxicity. • Recommend clothing (hats, etc).
TANNING • Tan Accelerators • Contain tyrosine - necessary for production of melanin, no evidence to support efficacy • Sunless Tanners • Dihydroxyacetone darkens outermost layer • Use at night, sunscreen during day • Tanning Booths • Newer types use light source composed of 95% UVA, < 5% UVB (even 1% may increase incidence of skin cancer).
PHOTOSENSITIVITY REACTIONS • Photoallergic Reactions • Radiation alters drug, becomes antigenic or acts as hapten. • Requires previous exposure. • Not dose related. • Induced by chemically related agents. • Eruption may present as urticarial, eczematous, bullous, or sunburn-like reactions. • Usually caused by topical agents.
PHOTOSENSITIVITY REACTIONS • Phototoxic Reactions • Radiation alters drug to toxic form, causes tissue damage. • Does not require previous exposure. • Dose related. • No cross-sensitivity. • Within several hours of exposure - appears as exaggerated sunburn.
CHOOSING SPF RATING HIGH SPF SUNSCREENS • Can achieve higher SPF by combining two or more agents. • SPF 30 (3%) vs 15 (6%) of radiation penetrating skin.
SUNSCREEN PRODUCTS PABA/Ester Oxybenzone Other Coppertone yescinnamate PreSun yesyes Bull Frog yescinnamate Q.T. Quick Tanning cinnamate Formula 405 Solar Lotion cinnamate
OTC BURN THERAPY • Burn Depth • First degree erythema, no blistering • Second degree erythema and blisters • Third degree No blisters, leathery white, mottled • Fourth degree “Charred”
Minor Burns: Second degree burn Third degree burn excludes electrical or inhalation injuries and all poor risk patients. < 15% BSA (10% in children) < 2% BSA not involving eyes, ears, face, hands, feet, or perineum). CLASSIFICATION OF BURNS (American Burn Association)
Estimation of Burned Area Rule of nines Body Area • Head 9% • Arm 9% • Leg 18% • Anterior Trunk 18% • Posterior Trunk 18% • Perineum 1%
OTC Treatment of Minor Burns/Sunburns • Ice/cool water • Cleansing - water and nonirritating soap • Dressings (usually only for second degree burns) • Nonadherent primary layer of sterile fine-mesh gauze • Absorbent intermediate layer to draw and store exudate • Supportive outer layer of rolled gauze bandage
OTC Rx of Minor Burns/Sunburns Local Anesthetics - short-term relief of pain • Benzocaine 5-20% (eg, Americaine®) sensitivity rxn; no systemic effects • Lidocaine 0.5-4% (eg, Bactine®) • Very low incidence of sensitivity rxn, but systemic toxicity may occur if applied to damaged skin or over large areas • Dibucaine 0.25-1% (eg, Nupercainal® Cream) • Tetracaine 1-2% (eg, Pontocaine®) • Pramoxine 1% (eg, Tronothane®) • Topical Antibiotic (Bacitracin, Polymixin-B Oint.) • Protectant (Sterile Petrolatum) - protects against mechanical irritation and aids rehydration of stratum corneum. • ASA for sunburns may help minimize inflammatory response.
POISON IVY/OAK/SUMAC • Allergen: • Urushiol is common to all of these plants • Transmission: • Contact with resin causes sensitization; • may require as little as 1 mcg. • Direct contact with plant is NOT necessary. • Plant must be injured/bruised to expose resin; however requires very little friction to damage plant. • Contact with resin may occur from shoes, family pet, firewood, etc • weeks or months after initial exposure.
POISON IVY/OAK/SUMAC • Prevention: • Washing within 5-10 minutes may abort reaction except in highly sensitive individuals. • Resin penetrates skin rapidly and binds to skin proteins after which washing is useless • 1 mcg may initiate rash in sensitive individual
POISON IVY/OAK/SUMAC • Symptoms: • Lesions are asymmetric and localized to areas of contact • Itching, followed by erythema, edema, papules (blisters) • (serum is not contagious) • Onset usually within 24-48 hrs • Healing may take 2-3 weeks
POISON IVY/OAK/SUMAC • Treatment: • Weeping Lesions: • Aluminum Acetate (Burow's Soaks) applied 15-30 min BID-QID and/or • Aveeno bath (colloidal oatmeal) 2-3 times daily for 30 min • po antihistamines for severe pruritus • AVOID topical: antihistamines, anesthetics, zirconium • After lesions have dried: • Hydrocortisone CR 0.5% applied 4-6 times daily