Download
1 / 36
370 likes | 393 Views
Learn about the roles of Glossopharyngeal (CN IX) and Vagus (CN X) nerves in swallowing, somatosensory and autonomic functions, with clinical insights and neural pathway details.

E N D
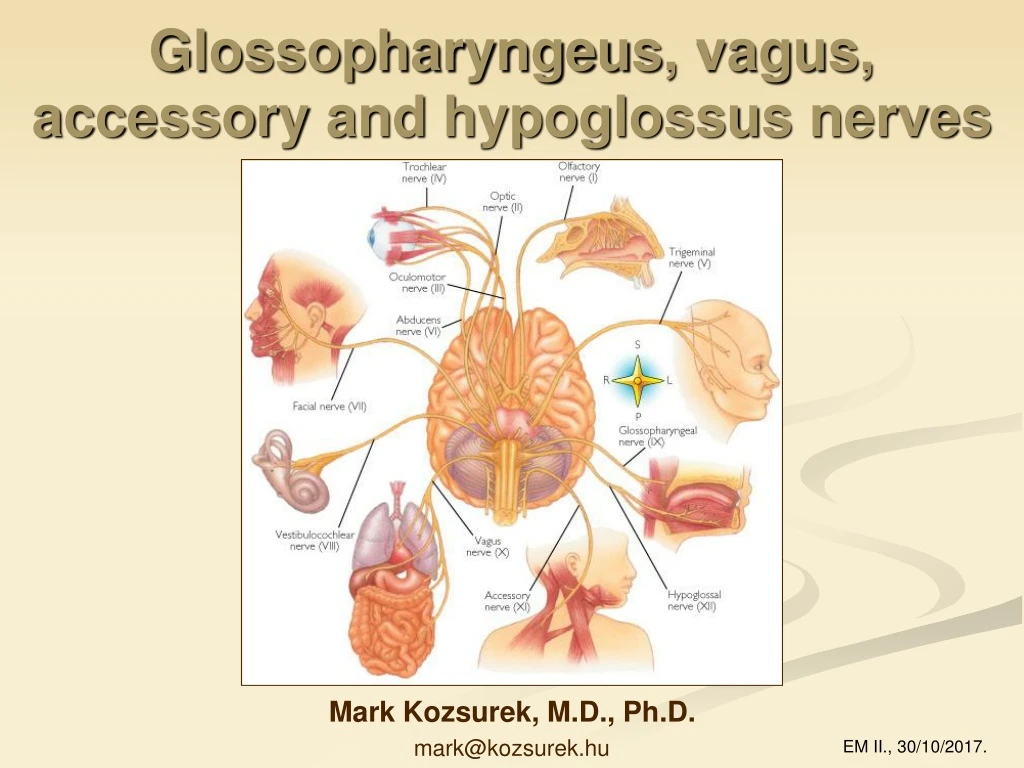
Glossopharyngeus, vagus, accessory and hypoglossusnerves Mark Kozsurek, M.D., Ph.D. mark@kozsurek.hu EM II., 30/10/2017.
Why is itgoodtohave a glossopharyngealnerve? • swallowing: Stylopharyngeus muscle, pharyngeal constrictor muscles • general somatosensory innervation: oral part of pharynx (e.g. sore throat!) • taste sensation: at the root of the tongue • salivation: parotid gland • blood pressure, pH, O2, CO2: carotid sinus and glomus Clinical consideration: Isolated damage of the glossopharyngeal nerve is rare and difficult to identify, as only some difficulty of swallowing might be present.
ambiguus nucl.: branchialmotor inferior salivatory nucl.: general visceromotor (parasympathetic) spinal trigeminal nucl.: general somatosensory solitary nucl. (caudal part) or lateral nucl. of ala cinerea:general viscerosensory solitary nucl. (rostral part):special viscerosensory (taste)
jugular gangl. petrosal gangl. At its cranial exit the glossopharyngeal nerve possesses two sensory ganglia with pseudounipolar neurons: the upper one is within the jugular foramen, pars nervosa, while the inferior one fits into the petrosal fossula. The first branch, the tympanic nerve ascends into the tympanic cavity through the tympanic canaliculus.
Tympanic nerve creates a plexus on the medial wall of the tympanic cavity together with those postganglionic sympathetic fibres which arrive along the internal carotid artery. Fibres of this plexus reunite to constitute the lesser petrosal nerve entering infratemporal fossa through the foramen lacerum.
Lesser petrosal nerve terminates within the otic ganglion found lateral to the mandibular division of trigeminal arriving into the infratemporal fossa through the foramen ovale. This is an autonomic ganglion with multipolar neurons which give arise to axons joining auriculotemporal nerve as guest fibres to reach the parotid gland.
Main trunk of the glossopharyngeal nerve further descends along the stylopharyngeus muscle (one of the levators of the pharynx) innervates this muscle and constitutes the pharyngeal plexus together with the branches of the vagus nerve and postganglionic sympathetic fibres derived from the superior cervical ganglion.
While descending along the pharyngeal wall gives off branches to the isthmus of the fauces, the palatine tonsils and the root of the tongue (tonsillary and lingual branches).
The most caudally descending fibres terminate close to the bifurcation of the common carotid artery where they innervate the carotid glomus and sinus (Hering nerve!)
Whydoweneedthevagusnerve?(Whatarethesymptomesinvagusinsufficiency?)Whydoweneedthevagusnerve?(Whatarethesymptomesinvagusinsufficiency?) • swallowing: Levator veli palatini muscle, pharyngeal constrictors, esophageal muscles • phonation: laryngeal muscles • viscera: lungs, heart, esophagus, stomach, liver, biliary system, pancreas, small and large intestine, kidney Clinical symptomes: dysphagia, aspiration, dysphonia, deviation of uvula.
ambiguus nucl.: branchialmotor dorsal vagal nucl.: general visceromotor (parasympathetic) spinal trigeminal nucl.: general somatosensory solitary nucl. (caudal part) or lateral nucl. of ala cinerea:general viscerosensory solitary nucl. (rostral part):special viscerosensory (taste)
I. Branchesonthehead and neck Posteriormeningealbranch Auricularbranch of vagusnerve superiororjugularggl. inferiorornodoseggl. 1. Posterior meningeal branch 2. Auricular branch of vagus nerve inferoposterior wall of the external auditory meatus, posterior surface of the auricle (mastoid canaliculus: jugular fossa → tympanomastoid fissure) Both of these branches contain exclusively general somatosensory fibres!
PHARYNGEALPLEXUS 1. Post. meningeal branch 2. Auricular branch 3. Pharyngeal branches
4. Superiorlaryngealbranch - externalbr.(Cricothyroid m.) - internalbr. 5. Inferior and recurrentlaryngeal nerve 1. Posterior meningeal branch 2. Auricular branch 3. Pharyngeal branches
6. CARDIAC PLEXUS - superior cervical cardiac branches - inferior cervical cardiac branches - (thoracic cardiac branches)
II. Thoracicbranches • thoracic cardiac branches • bronchial branches • pericardiac branches • esophageal branches
III. Abdominalbranches * Cannon-Böhm’s point • gastric plexus • hepatic plexus • celiac plexus • renal plexus The most distal branches follow the celiac trunk and the superior mesenteric artery to reach their targets.
posterior meningeal br.: general somatosensory auricular branch of vagus nerve: general somatosensory rr. pharyngei: branchialmotor (striated muscles), general visceromotor (glands), general somatosensory (mucosa) superior laryngeal nerve: external br. – branchialmotor; iternal br. – general somatosensory (mucosa), special viscerosensory (taste sensing), general visceromotor (glands) fibres inferior and recurrent laryngeal nerve: branchialmotor, general somatosensory (mucosa), general visceromotor (glands) abdomen thorax head, neck cardiac plexus: general visceromotor and viscerosensory (blood pressure, heart rate) bronchial, pulmonary, pericardiac and esophageal plexus: general visceromotor and viscerosensory gastric, coeliac, hepatic, renal plexus: general visceromotor and viscerosensory
General viscerosensory and visceromotorfunctions of thevagusnerve • Vagus controls the autonomic functions of the thoracic and abdominal viscera. inferior ganglion (pseudounipolar neurons) lateral nucleus of ala cinerea (caudal part of the solitary nucleus) viscera dorsal vagus nucleus parasympathetic (intramural) ganglia submucous and myenteric plexus multipolar neurons
Whatdoestheaccessorynervedo? • phonation: fibres joiningthevagusmainlyinnervatetheinterarythenoidmuscles. • innervation of trapezius and sternocleidomastoidmuscles Clinicalsymptoms: abnormal, asymmetrical position of thehead or neck („wryneck”), abduction of theupperlimb over thehorizontalplane is difficult.
ambiguusnucleus: branchialmotor (fibres arisingfromthisnucleusconstitutethecranialrootswhichexit in thelateralparolivarysulcus and thanjointhevagusnerveasinternalbranches) spinalaccessorynucleus:general somatomotornucleusinthelateralportion of theventralhornof C1-C6 spinalsegments. (fiberscomingfromthenucleusgivethespinalrootsof theaccessorynervewhich enter theskullthroughtheforamenmagnumexit again throughtheparsnervosa of thejugularforamen and targetsternocleidomastoid and trapeziusmusclesasexternalbranches)
glossopharyngeus nerve vagus nerve
Functions: 1. Somatomotor innervation of extrinsic and intrinsic muscles of the tongue. 2. Contributes to the innervation of infrahyoid muscles (and the geniohyoid) by taking guest fibres from the cervical plexus. hypoglossal nucleus: general somatomotor
Clinical consideration: Peripheral injury of the hypoglossal nerve results in deviation of the protruded tongue toward the side of injury. Tongue might be atrophic. Chewing, swallowing, talking is difficult.
deep cervical ansa: a branch of C1 spinal nerve joins the hypoglossus as a guest fibre and later leaves that as the superior root of cervical ansa. This will form a loop with the inferior root of ansa cervicalis arrising from the ventral branches of C2-3 spinal nerves. Deep cervical ansa innervates infrahyoid muscles and the Geniohyoid.
Pirogov’striangle is formedbythe intermediate tendon of the digastric muscle, the posterior border of the mylohyoid muscleand the hypoglossal nerve. Béclard's triangle is an area whose boundaries are the posterior border of the hyoglossus, the posterior belly of the digastric/stylohyoid muscles and the greater horn of the hyoid bone.
Hypoglossus nerve is found in the lateral sulcus of the tongue bellow the lingual nerve and the submandibular duct.