Download
1 / 19
190 likes | 382 Views
Management of Violence in the Emergency Department. by Dr Sharon Fish. Overview. Violence in the Emergency Department Gangs Recognition of gangs & potential for violence Causes of violence & the emergency room Violence Management Physical methods Protocols & Procedures Case Studies

E N D
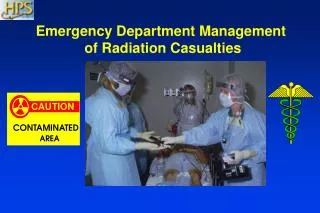
Management of Violence in the Emergency Department by Dr Sharon Fish
Overview • Violence in the Emergency Department • Gangs • Recognition of gangs & potential for violence • Causes of violence & the emergency room • Violence Management • Physical methods • Protocols & Procedures • Case Studies • Focus Groups • Sport / Crowd violence • Local effects • Discussion
Prevalence – Emergency Department • ED often first point of entry • Intoxication, concealed weapons and stress potentially all present at the same time • Research suggests that staff in the Emergency Department receive the most amount of verbal and physical abuse out of any other department. • Nature of the work implies exposure to violence, so methods of violence management are vital
Gangs • Socio-economic unbalance • unequal distribution of wealth • societal exclusion • poor education • Means of expressing an identity outside of the status quo • Crime - easiest access to rewards and goals • drugs as the economy. • May include entire families, yet can lead to unfair stereo-types of communities or racial groups.
Western Cape Gangs • Street gangs • the Americans • the Hard Livings • the Sexy Boys • the School Boys • the Junky Funky Kids (JFK) • Young Dixie Boys (YDB) • Prison Gangs • 26’s, 27’s, 28’s • Tatoo’s indicating rank
Recognition of Violence • Aggression • towards an individual • toward creating fear • Stress behaviours in individuals include • use of profanity and verbal outbursts • pacing or frequent alteration of body position or posture • indicate increasing agitation
Recognition of Gangs • Awareness of the local gang culture • Access this information from local law enforcement • Distinctive markings & behaviours • Observe when gang members are present in hospital • Security must be aware of an injured gang member arriving • Types of injuries should be noted. • Rivals may visit the hospital to finish their job • Volatile in group or if rival gang members are present
Causes of Violence • Not always gang related; and not all gang members are violent in certain situations (i.e. child birth) • Understand root of behaviour • psychiatric • drug induced (either intoxication or withdrawal) • child, elder or spousal abuse • frustration due to long waits, unrealistic expectation
Causes of Violence • Overcrowding • Creates volatile situations • Increased wait times • Neglect of patients who require urgent attention • Proximity of rival groups • gangs • intoxicated driver in close proximity to victims
Management throughPhysical Methods • Access control • Minimised unguarded entrances; lock extraneous entrances / exits at night • Secure sensitive areas with access control • Hand-held metal detectors used by security • Enforce visible identification of all staff • Plexiglass between waiting room & ED dept • Block unauthorised vehicle access to the emergency department • Visible security inside & outside
Management throughPhysical Methods • Rankins and Hendey suggest that removing weapons did not decrease number of assaults • Training of ED staff to handle violent situations remains crucial
Management throughProtocol & Procedure • Develop a safety plan with hospital security • Rehearse response mechanisms • Code word called out when violence erupts • Close contact with law enforcement during high-volume or disaster management scenarios • Debrief after major incidents to refine procedures • Access patient history either by records, friends or family to gain proper perspective on a patient • Undress patients to reveal concealed weapons and disarm if necessary
Management throughProtocol & Procedure • Security should recognise an escalating situation • Either between parties or individual misconduct • Separate rival gang members or victim-perpetrator groups • Do not show condescension towards gang members. Cultural differences and language barriers may already cause tension • Immediately use chemical and/or physical restraints with sufficient personnel
Case Study – Leven et al. • Insights of nurses about assault in hospital-based emergency departments on subjective factors to reduce risk of assault • Personal • attitude & body language determine respect given by patients • Workplace • security must be trained to recognise and defuse violent situations • authoritatively uniformed security who perform proactive, visible patrols perceived as more effective than more casually dressed security that respond reactively • Geographic location • Determines the type of incidents that occur • Perception that police default to bringing intoxicated individuals to the emergency department as a holding area until they sober up
Case Study – Soccer Violence • Winterbottom describes soccer players who arrive at casualty in a group • Patients with minor injuries become belligerent because they must wait their turn, but at the same time want to get back to the remainder of the match • In conjunction, patients escorted by their healthy friends cause disruption, worsened if supporters of the opposing team are present • Describes violence and aggression as being rooted in frustration, fear and anger
Closer to Home – Security Upgrade at Livingston Hospital • Gun wielding gangs • attacked patients, security staff & rival gang members • patient shot dead during surgery • September 2007 - Nurses robbed at gun point at Dora Nginza Hospital, Tower Psychiatric Hospital in Beaufort West. • Stated Solutions • CCTV cameras • Swipe card system for maternity wards & ICU
Discussion • Personal Perspectives / Experience • Long term effects of violence experienced on staff morale and performance • Continuous process of managing violent behaviour and associated reactions • Which security strategy carries most weight: physical or procedure-based security measures?
References • Irvin Kinnes, The Future, Gangs and Society. Monograph No 48, From urban street gangs to criminal empires: The changing face of gangs in the Western Cape, June 2000. • Irvin Kinnes, Gang culture in South Africa and its Impact, Institute of Criminology, University of Cape Town. • McAcams, Russell, Walukewcz, Gangstas – not in my hospital!, Nursing 2004, Volume 34, Number 9, September 2004. • Robert W. Derlet, John R. Richards , Overcrowding in the Nation's Emergency Departments: Complex Causes and Distrurbing Effects, Annals of Emergency Medicine, Volume 35, Number 1, January 2000. • Ordog et al, Violence and General Security in the Emergency Department, Academic Emergency Medicine, February 1995, Volume 2, Number 2. • Beth R. Keely, Recognition and Prevention of Hospital Violence, Dimensions of Critical Care Nursing, Volume 21, Number 6, 2002. • Robert C. Rankins, Gregory W Hendey, Effects of a Security System on Violent Incidents and Hidden Weapons in the Emergency Department, Annals of Emergency Medicine, Volume 33, Number 6, June 1999. • Pamela F. Levin, Jeanne Beauchamp Hewitt, Susan Terry Misner, Insights of nurses about assault in hospital-based emergency departments, Journal of Nursing Scholarship, 1998. • Department of Health, Easter Cape Provincial Government, http://www.ecdoh.gov.za (2008) • Sylvia Winterbottom; Coping with the violent patient in accident and emergency. Journal of medical ethics, 1979, 5, 124-127.