Download
1 / 44
440 likes | 619 Views
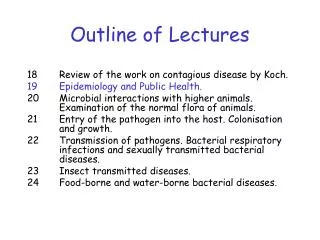
Outline of Lectures. 18 Review of the work on contagious disease by Koch. 19 Epidemiology and Public Health. 20 Microbial interactions with higher animals. Examination of the normal flora of animals. 21 Entry of the pathogen into the host. Colonisation and growth.

E N D
Outline of Lectures 18 Review of the work on contagious disease by Koch. 19 Epidemiology and Public Health. 20 Microbial interactions with higher animals. Examination of the normal flora of animals. 21 Entry of the pathogen into the host. Colonisation and growth. 22 Transmission of pathogens. Bacterial respiratory infections and sexually transmitted bacterial diseases. 23 Insect transmitted diseases. 24 Food-borne and water-borne bacterial diseases.
Epidemiology • Study of occurrence, distribution, and control of diseases within populations. • Infectious disease control has been extremely successful in developed countries (see previous lecture) • However, worldwide, infectious diseases are still responsible for 30% of 56 million annual deaths – a big problem especially for developing countries. • The developed world is also at risk (international travel, climate change, etc). • New infections like West Nile fever are emerging and diseases like TB are reemerging. • Scientific, medical, economic, educational solutions are required to keep infectious diseases under control.
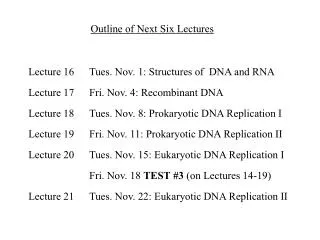
Microorganisms and Disease in the USA 2008 1900 Influenza and pneumonia Heart disease 280 Cancer 205 Tuberculosis Stroke Gastroenteritis Pulmonary disease Heart disease Accidents Stroke Influenza and pneumonia Kidney disease Diabetes Accidents AIDS Cancer Suicide • Red: microbial disease Brock 12th ed. Fig. 1.8 • Green: non-microbial disease Cirrhosis of the liver Infant diseases Diphtheria Homicide 100 200 0 0 100 200 Deaths per 100,000 population Deaths per 100,000 population
Deaths caused by infectious disease in the USA • A general decrease throughout 20th century. • Why a spike at 1918? • A significant increase in infectious disease mortality from 1980 onwards
Pathogens • Pathogens often kill the host – if so why doesn’t the pathogen become extinct? • A pathogen must grow and reproduce in the host in order to cause disease. • Pathogens can be host-dependent or host-independent for survival. • A well adapted pathogen lives in balance with host leading to a chronic (long-term) infection. When there is equilibrium between host and pathogen, they both survive, however if the host’s defence is low due to poor diet, age and other factors, then the host might get damaged.
Pathogens A newly arisen pathogen may cause more serious infection – such a situation may arise when a species barrier is crossed (e.g. bird flu, swine flu). Such pathogens usually cause acute infections. In these cases, both the pathogen and the host play an important role in each other’s evolution. • In some cases, the pathogen might not depend on the host for survival. Organisms of the Clostridium genus live in soil but may accidentally infect humans (tetanus or botulism). In this case, the death of the temporary host will not affect general survival of the pathogen.
The epidemiologist • Traces the spread of disease. • Determines the origin of disease and mode of transmission. • Gathers data from: • Clinical studies • Disease reporting surveys • Insurance questionnaires • Patient interviews • Aim is to define common factors that constitute a disease in order to improve and maintain public health measures and effectively control disease.
Epidemiological terms • Prevalenceof disease: Proportion of diseased individuals in a population in a given period of time • Incidence of disease: Number of new cases of disease in a given period of time • Epidemic: Unusually high number of diseased individuals occurring in a population at the same time • Pandemic: Widespread, usually worldwide epidemic • Endemic: Low incidence but constant presence of disease in a population
Epidemiological terms (cont.) Sporadic cases of disease: Individual cases of disease that occur in a scattered manner. Outbreak: A sudden increase in the number of disease cases in a relatively short period of time. Subclinical infections: Infections where the diseased individuals show mild symptoms or no symptoms at all. Carriers: Individuals subclinically infected – showing few or no symptoms. They maybe actively carrying and spreading the pathogen. http://www.microbiologyplace.com – Epidemiology: Occurrence of Diseases
Mortality and morbidity • Mortality • The incidence of death in a population • Morbidity • The incidence of disease (fatal and non-fatal cases). • Many diseases cause illness but not death. Thus morbidity statistics reflect the status of the general health of a population better http://ps4h.org/communicable_diseases.html Morbidity Rates for Poliomyelitis in Cuba http://www.medicc.org/publications/medicc_review/I/varied/html/inmuno.html
Typical progression of disease for microbial infections • Infection – organism invades, colonises and grows in host • Incubation period- time period between infection and symptoms (depends on organism virulence, inoculum size, host defence status, distance between entrance site and target site. Towards end of incubation symptoms appear . • Acute period - height of disease (fever, aches etc) • Decline period - symptoms subside • Convalescent period - return to normal health
Reservoirs of disease and epidemics • A reservoir is a site where infectious agents are located • Reservoirs might be animate or inanimate (see next two slides or table 33.2 in Brock) • A number of pathogens require a living organism (humans and/or animals) as a reservoir for their existence. These (especially pathogens that live only in humans) can usually be controlled and even be eradicated. • On the other hand, some pathogens are saprophytic and only incidentally infect humans and cause disease. These pathogens, therefore do not need to infect a host for survival. • E.g. Clostridium tetani – causative agent of tetanus, normally inhabits soil. - Zoonosis: A disease that primarily infects animals, but occasionally transmitted to humans. E.g. SARS, bird-flu, swine-flu.
Disease carriers • A carrier is a pathogen infected individual that has no obvious signs of disease. • They might be at incubation stage of disease – acute carriers. • Chronic carriers may be infected for long periods with no outward symptoms and therefore may spread disease for extended periods of time. • Carriers can be identified by testing (culture or antibody). • Typhoid Mary (Mallon) was a cook in New York (early 20th century). She was probably a carrier of Salmonella typhi (typhoid). • Infected 47 people – 3 died! She rejected all accusations that she might be responsible. • She was eventually imprisoned because she refused to have her Gall bladder removed.
Infectious disease transmission • Epidemiologists correlate infection with season, geography, age group etc. • California encephalitis rises in summer and falls in winter (mosquito borne viral disease). • Disease follows mosquito prevalence
Infectious disease transmission • Host to host transmission is the key to pathogen survival. • Pathogens can be classified by their transmission mechanisms (direct or indirect), which have 3 stages in common: (1) Escape from host (2) Travel (3) Entry into a new host
Infectious disease transmission Direct host-to-host transmission: Direct transmission of infection to a susceptible host by an infected host without the assistance of an intermediate agent. E.g. Flu (influenza virus), common cold (rhinoviruses), STIs (syphilis – Treponema pallidum; gonorrhea – Neisseria gonorrhoeae), boils and pimples (staphylococci), ringworm (fungi) . Droplets resulting from sneezing or coughing most often cause direct transmission of upper respiratory tract infections such as flu and the common cold.
Infectious disease transmission Indirect host-to-host transmission: Transmission of infection to a susceptible host by an infected host with the assistance of an intermediate agent (living or nonliving). Living agents are called vectors. E.g. arthropod insects or vertebrates. Nonliving/inanimate agents are called fomites and these include bedding, toys, books, cutlery, surgical instruments. Food and water are potential disease vehicles.
Common source epidemics • Arises due to infection of a large number of people from a contaminated common source (food, water supply). • Foodborne and waterborne common source epidemics; intestinal diseases - pathogen leaves the body in faecal material, contaminates food or water supplies, enters the intestinal tract of the recipient during ingestion. • Classic example is cholera – faecal contamination of drinking water. Vibrio cholerae is the infectious agent. • Usually a common source epidemic has a rapid rise to peak (simultaneous infection) Cholera ward in Bangladesh http://www.microbiologyplace.com – Epidemiology: Transmission of Disease
Host-to-host epidemics • Typically has a slow progressive rise and a gradual fall. • Might be initiated by a single infected person in a population. • Pathogen spreads to susceptible individuals where it replicates and is spread to other susceptible individuals. • Influenza and chickenpox are examples of diseases that are typically spread in host-to-host epidemics. Flu epidemic Chicken pox blisters
Herd Immunity • Resistance of a group to infection due to immunity of a high proportion of its members. • Must assess immune state of population. • If a high enough proportion are immune then whole population is effectively protected. • If immunity is absent, even poorly infective agents can be transmitted person-to-person. E.g. H5N1 avian influenza cases in humans. • Need data from immunization programmes to estimate the proportion of population that is immune in order to prevent infection in the rest of the population. • Polio: if 70% immunized then all population is protected but depends on population density – this % depends on transmissibility (e.g. chickenpox needs 90% immunization). • Sometimes, immunized people can be carriers e.g. diphtheria. This is due to immunisation being protective against the effects of diphtheria toxin, but not necessarily against its causative agent Corynebacterium diphtheriae.
Herd immunity Infected person (red) transmits disease to susceptible people (blue). Immunized people (yellow) prevent spread and thus protect person B and C.
Epidemiology and public health • Identification, containment and eradication of disease. • Public health refers to the health of the general population and the measures taken by public health authorities in the control of disease. • Improvement of basic living conditions (sewage treatment, clean drinking water, better nutrition, less cramped living- all help). • Quarantine and vaccination have played a major role in controlling several diseases, including small pox, typhoid fever, diphtheria, poliomyelitis
Control of disease • Control the reservoir • Domestic animals – treat, immunise • Wild animals – eradicate (badgers, bovine TB) – more difficult • Rabies would require elimination of all wild animals! • Insect (mosquito) – insecticides – but environmental risks. • What if reservoir is human (e.g. HIV or TB)? – quarantine, control spread, immunise if possible. Strategy used for eradication of smallpox successfully and is currently being used for eradication of polio.
Control of disease • Transmission control • Pathogens in food or water eradicated by treatment (example is milk pasteurization and control of bovine TB in humans). • Respiratory pathogens more problematic – air filtration not feasible. Face masks (Japan)
Control of disease • Immunization • Many diseases have been controlled by immunization (e.g. Smallpox, diphtheria, tetanus, pertussis, measles, mumps, rubella, polimyelitis) • 100% immunization not necessary (herd-immunity) • Vigilance must be ensured to ensure appropriate level of immunization. Complacency a problem. Due to decline of immunity over time, a high percentage of adults lack effective immunity to important infectious diseases. Therefore, update of immunity in adults (boosters – 10 years) - a necessary measure in controlling disease. • Autism scare in UK from MMR – probably unfounded but now measles on rise due to low uptake of vaccination.
Control of disease • Quarantine • Restricting the movement of infected individuals until they are no longer infectious. • Time-limit will be the longest period of communicability of that disease. May simply mean the individual stays at home when infected. • Isolation may be used for severe infectious diseases. • International agreement for quarantine include: Smallpox, cholera, plague, yellow fever, typhoid fever, relapsing fever.
Control of disease • Surveillance • Observation, recognition, reporting of disease. • The list might change and will vary from season to season and from country to country. • CDC – centre for disease control and prevention through the National Centre for Infectious Diseases (NCID). • National databases are formed through reported diseases, which are then used to formulate and implement plans for isolation, diagnosis, treatment and to stop their spread.
Control of disease • Pathogen eradication • Aim is to remove all of a pathogen from any reservoir. • Several pathogens have effectively been eradicated by immunization programmes (WHO eradicated smallpox 1980) • Polio eradicated from Western hemisphere using same strategy. • Leprosy is targeted and can be treated by multidrug therapy • Chagas’ disease (Trypanosoma cruzi) elimination underway by vector control and treatment of active cases.
Emerging and Reemerging Infectious Diseases • Worldwide disease distribution changes rapidly. • Emerging diseases are those that suddenly become prevalent. E.g. syphilis, plague, legionellosis, AIDS and Lyme disease. • Reemerging diseases are those that have become prevalent after having been previously under control. E.g. TB • See Table 33.8 in Brock.
Emerging and Reemerging Infectious Diseases • Emergence Factors • Human demographics and behavior • Technology and industry • Economic development and land use • International travel and commerce • Microbial adaptation and change • Breakdown of public health measures • Abnormal natural occurrences
Emerging and Reemerging Infectious Diseases • Addressing emerging diseases: • Recognition of disease • Surveillance • Intervention to prevent pathogen transmission • - In order to isolate outbreaks and prevent spread of specific diseases; quarantine, immunisation and drug treatment must be employed as means of public health response. • Vectorborne and zoonotic diseases, the animal host or vector must be identified, life cycle of the pathogen must be interrupted and transmission to humans must be prevented. E.g. Controlling the emergence of SARS
Directed Reading: • Hughes J. M. 2001. Emerging Infectious Diseases: A CDC Perspective. Emerging Infectious Diseases, 7, 494-496. • Madigan et al., 2009. Brock (12th ed). Chap.33
Biological Warfare and Biological Weapons • Biological warfare is the use of biological agents to kill a military or civilian population • Biological weapons are organisms or toxins that are • Easy to produce and deliver • Safe for use by the offensive soldiers • Able to incapacitate or kill individuals under attack in a consistent and reproducible manner
Anthrax as a Biological Weapon • Bacillus Anthracis is a preferred agent for biological warfare and biological terrorism • Endospores enhance ability to disseminate B. anthracis in aerosols • Three forms of the disease • Cutaneous anthrax • Gastrointestinal anthrax • Pulmonary anthrax
Anthrax as a Biological Weapon • Weaponized Anthrax • Refers to preparations of B. anthracis that exhibit properties to enhance dissemination • Vaccination is only done on people at risk • Treatment of anthrax is done with Ciprofloxacin • Small particle size interspersed with a very fine particulate agent (usually talc)
Cutaneous Anthrax Inhalation Anthrax