Download

1 / 48
480 likes | 636 Views
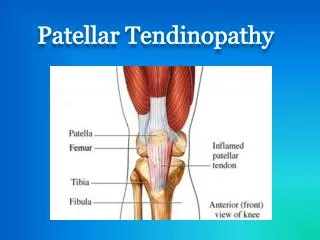
A Comprehensive Approach in the Management of Patellar Tendinopathy. Eric Greenberg, PT, DPT, CSCS Sports Medicine and Performance Center at The Children’s Hospital of Philadelphia King of Prussia, PA. Patient History. 15 year old male 10 th grade Sports - Soccer and Basketball

E N D
A Comprehensive Approach in the Management of Patellar Tendinopathy Eric Greenberg, PT, DPT, CSCS Sports Medicine and Performance Center at The Children’s Hospital of Philadelphia King of Prussia, PA
Patient History • 15 year old male • 10th grade • Sports - Soccer and Basketball • Rx: Bilateral Patellar Tendinitis • Evaluate and Treat • Chief Complaint • Bilateral anterior knee pain R > L
Subjective response • Onset of Symptoms • Present for 2 years- no isolated event • Pain Levels • Current - 0/10 while sitting; Worst -10/10 • Described pain to midsubstance of patella tendon as sharp/stabbing • Increases with running, jumping, bending knee, prolonged standing, kneeling • Decreases with rest, inactivity, and Advil • Daily occurance especially at the end of the day • Recent changes in activity • Increased intensity/duration of basketball practice since entering high school • Growth spurt 2 years ago- he is now 6’3” tall • Prior Treatment • Use of OTC arch supports • 4 sessions of PT - All modalities and was told “PT will not benefit him” • Physician recommended surgical debridement of tendon • Diagnostic Imaging • Plain Radiographs- fully closed physes • MRI- R knee- increased signal in proximal patella tendon and infrapatellar fat pad • PMH • Sever’s Disease- 2 years ago; Ankle fx- 1 year ago
What is the significance of his skeletal maturity? A. Tendon is more prone to overuse in the skeletally immature B. Bone is more prone to overuse in the skeletally immature C. Bone and tendon are equally at risk for overuse in the skeletally immature D. Point me to the ultrasound!
Functional Limitations • Unable to stand > 10 minutes continuously • Unable to ambulate greater than 10 minutes without pain to B knees • Unable to participate in Winter Basketball • International Knee Documentation Committee (IKDC) Subjective Knee Score • 47.13
IKDC Subjective Knee Score • Subjective pain and functional outcome measure • A score of 100 = no limitation with activities of daily living or sports activities and the absence of symptoms • Used for patients with meniscal pathologies, ligamentous instability and generalized knee pain • Minimal Detectable Change • 11.5 points • Minimally Clinically Importance Difference • 20.5 points
Goals • Patient Goals • To return to JV basketball sometime during the Winter season without limitations from pain • Short Term Goals • Pt will be able to negotiate 2 flights of steps reciprocally without pain or compensation within 4-6 weeks • Pt will be able to ambulate for 10 continuous minutes before onset of anterior knee pain within 4-6 weeks • Long Term Goals • Pt will be able to run for 10 minutes continuously without onset of knee pain in preparation for progressive return to sport within 12-14 weeks • Pt will be able to play in a basketball scrimmage for 10 consecutive minutes without diffculty due to knee pain within 4 months.
Tests and Measures • Postural Assessment • B Hallux Valgus • B pes planus- dropped MLA height • B RF Valgus • B Squinting Patellae • Decreased R calf girth • Gait • Excessive R toe out • Increased tibial IR • L Trendelenburg Sign • Tenderness to palpation • 5/10 B midsubstance patellar tendons • Thickening to B Patellar tendons • Effusion • None • Knee ROM • R: 2-0-152 (pain-free) • L: 2-0-150 (pain-free) • Flexibility • (+) Thomas Test • R ITB and RF • L HF • (+) Ober Test • R > L • (+) HS SLR • 60 degrees bilaterally • (+) Elys test • R only • (+) Gastroc length test • R DF KE/KF- 5/20 • L DF KE/KF- 7/20
Tests and Measures (cont’d) • Strength • Joint Mobility • ↓ STJ medial glide • Normal Posterior TCJ • Normal Patella mobility • Functional Testing • Single leg Stance • > 30 seconds bilaterally with Trendelenburg sign L > R • Bilateral Squat • ↑ LE pronation, medial collapse • Premature heel rise • Knees translate anteriorly to toes • Unilateral Squat • R and L - painful, ↑ medial collapse, heel rise • Lateral Step Down • B ↑ medial collapse, heel rise, trunk anterior lean • Bilateral Hop • ↓ eccentric control, knee flexion angles, ↑ medial collapse • Unilateral Hop • Same as bilateral hop but more pronounced • Unilateral Bridge • Unable to maintain level pelvis R > L
Impairment List • Pain • Muscle Flexibility • Muscle Strength • Neuromuscular control • Joint hypomobility
Tendinitis v. Tendinopathy • Tendinitis: an acute inflammation of a tendon due to increased mechanical loading or friction • Three stages of healing • Inflammation, proliferation, maturation • Tendinopathy: chronic tendon overuse that is non-inflammatory in nature that effects the histology of the tendon • “Failed healing process” • Does not follow healing process, resulting in long term disruption of extracellular matrix • Result: inability to absorb loads or transmit forces Peers, KHE and Lysens, RJJ, 2005 Kountouris, A. and Cook, J., 2007 • Which is more consistent with the patient’s presentation?
Rehabilitation Plan • Appropriate Duration of Treatment • Rarely shorter than 3 months • Maintenance of 6-12 months Kountouris, A. and Cook, J., 2007 • Fees for Services • Cost-effective • Insurance benefits • Time Management • High School Student/Athlete • Patient compliance
Rehabilitation Plan • Appropriate duration of treatment • Planned for 4-5 months of treatment • Stressed Home Exercise Program • Fees for Services • Total of 20 authorized PT visits over 5 month period • Initially seen 2x /week for 4 weeks • Decreased frequency to 1 x /wk for next 5 weeks • Decreased to 1x every 2 weeks for next 2.5 months • Time Management • Simplicity of HEP/ strategies for performance • Patient and parent education
Rehabilitation Program Components • Managing tendon pain and modification of tendon load • Exercise-based rehabilitation and adapting the tendon to increasing loads • Additional treatment options for tendinopathy
Managing Tendon Pain and Modification of Tendon Load Goal: To decrease reactivity to allow more active participation Which is NOT an example of how we can manage tendon pain or modify tendon loading? A. Activity modification/Active Rest B. Noxious e-stim C. Ice massage D. Progressive Resistive Exercise E. Bracing/Counter-force strapping
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Eccentric Strengthening • Decline squats increase mechanical loading to patellar tendon • Frohm, A. et al, 2007 • Initiated once pain more controlled • Week 2 • Decline squats and lateral step downs performed at each treatment • 3 sets of 15 each bilaterally • Allowed slight pain ~3/10 • Progressive loads • HEP always included lateral step downs done at least daily • Progressed weight with school backpack
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Question • Should we stop treating this patient and refer back to the physician since he is not showing any functional improvement in IKDC scores? • Yes • No
Remember...... • May not show functional gains for over 3 months Kountouris, A. and Cook, J., 2007 • Attempt conservative care for 6 months prior to more invasive procedures
Additional Treatment Options for Tendinopathy • What other treatments can be used in conjunction? • Iontophoresis • What solution/medication would you chose to utilize? • Dexamethasone 0.4% • Acetic Acid 5% • Lidocaine 4% • Sodium Salicylate 2%
Evidence on the Implications for Iontophoresis with Acetic Acid • Calcific deposits, MO, Frozen joints • Research mainly on plantar fasciitis and calcific shoulder tedinitis • Low level case studies Costa, IA and Dyson, A, 2007 • Plantar fasciitis and patellar tendinosis similarities • Overuse syndromes that develop over time as a result of repeated stress and exceeds body’s ability to repair itself • Non-inflammatory, chronic conditions (-osis) • Use of Acetic Acid ionto is promising within 3-4 weeks and over 2 yr follow up • Chronically inflamed tissue results in ↑ concentrations of insoluble calcium carbonate • Ongoing pain cycle and abnormal restructuring of tissue • Acetate ion combines with calcium ion to form a more soluble calcium acetate to dissolve within blood circulation
Issues and Concerns re: use of Iontophoresis • Limited number of Authorized Visits • Possible home application? • Obtaining supplies • Costs • Perform bilaterally or unilaterally?
Question • Which of these is NOT an issue to consider when recommending a patient administer iontophoresis independently at home? • The patient’s age • Use of a syringe • Possibility of skin irritation • Contamination of solution • All of the above are issues to consider
How We Made It Happen! • Obtained Rx for Empi Action Patches • Mobile iontophoresis delivery system • Can be used at home for 3 hours a treatment • Light goes on to signify activity of treatment that will automatically turn off once complete • Contacted pharmacy • Needless syringes • Sterile vile • Patient and Mother education • Mother administered all treatments
Frequency of Ionto • Some literature recommends administration 2-3 x week • Performed every other day for a total of 8 treatments on each limb • Instructed to keep on for 3 hours after light turns off • Attempted 4 dosages on left knee before attempting on right • Effectiveness based upon subjective reports of pain
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Exercise-Based Rehabilitation and Adapting the Tendon to Increasing Loads
Sport-Specific Activities (Week 14) Hurdles Fwd/lat Fwd/lat Unilateral Hops Squat Jumps Cycled Split Squat Jumps Pivotting/ Cutting Activities
Outcomes • Able to manage conservatively without surgery • Progressed in PT over last 5 visits to full return to competitive basketball in time for last few games of season • 0/10 pain at D/C • Worst : occasional 2/10 pain with basketball • Good control with landing and jumping activities without complaints of pain • Functional hop test • Symmetrical strength to hips and quads • Improved overall flexibility • Only minor limitations to gastrocs, HS, ITB
Clinical Pearls • Everyone is not seen just 3 times a week for 6 weeks • Should be individually based • Empower your patient!! • Active role in therapy • Patient education is vital • Fear of the unknown • Helps establish trust • Be an advocate for your patient • Go the extra mile • Treatment should be multifactorial and complete • See it through to the end
References • Alfredson, H and Lorentzdon, R. Chronic Achilles Tedinosis: Recommendationd for treatment and prevention. Sports Medicine Feb 2000, 29(2), 135-146. • Costa, IA and Dyson, A. The integration of acetic acid iontophoresis, orthotic therapy and physical rehabilitation for chronic plantar fasciitis: a case study. J Can Chiropr Assoc 2007, 51 (3),166-173. • Guy, RH. Iontophoresis- Recent develpments. J Pharm Pharmacol 1998, 50, 371-4. • Japour, CJ, Vohra, R, Vorha, PK, Garfunkel, L, Chin, N. Management of heel pain syndrome with acetic acid iontophoresis. Journal of the American Podiatric Medical Association May 1999, 89 (5), 251-7. • Koen, HE and Lysens, RJJ. Patellar Tendinopathy in Athletes: Current diagnostic and Therapeutic recommendations. Sports Medicine 2005. 35(1), 71-87. • Kountouris, A and Cook, J. Rehabilitation of Achilles and Patellar tendinopathies. Best Practice & Clinical Rheumatology 2007, 21(2), 295-316.