Download
1 / 2
20 likes | 104 Views
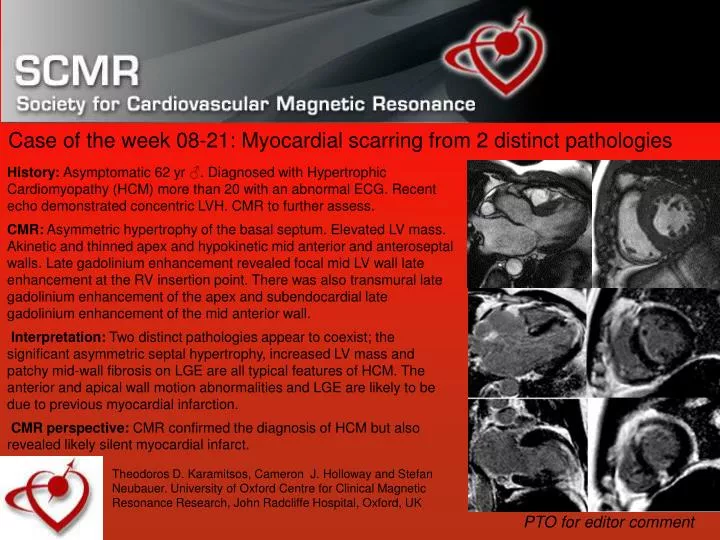
History: Asymptomatic 62 yr ♂. Diagnosed with Hypertrophic Cardiomyopathy (HCM) more than 20 with an abnormal ECG. Recent echo demonstrated concentric LVH. CMR to further assess.

E N D
History: Asymptomatic 62 yr ♂. Diagnosed with Hypertrophic Cardiomyopathy (HCM) more than 20 with an abnormal ECG. Recent echo demonstrated concentric LVH. CMR to further assess. CMR:Asymmetric hypertrophy of the basal septum. Elevated LV mass. Akinetic and thinned apex and hypokinetic mid anterior and anteroseptal walls. Late gadolinium enhancement revealed focal mid LV wall late enhancement at the RV insertion point. There was also transmural late gadolinium enhancement of the apex and subendocardial late gadolinium enhancement of the mid anterior wall. Interpretation:Two distinct pathologies appear to coexist; the significant asymmetric septal hypertrophy, increased LV mass and patchy mid-wall fibrosis on LGE are all typical features of HCM. The anterior and apical wall motion abnormalities and LGE are likely to be due to previous myocardial infarction. CMR perspective: CMR confirmed the diagnosis of HCM but also revealed likely silent myocardial infarct. Case of the week 08-21: Myocardial scarring from 2 distinct pathologies Theodoros D. Karamitsos, Cameron J. Holloway and Stefan Neubauer. University of Oxford Centre for Clinical Magnetic Resonance Research, John Radcliffe Hospital, Oxford, UK PTO for editor comment
Case of the week 08-21: Myocardial scarring from 2 distinct pathologies Editor comments: This case caused some debate. 3 of 4 COTW editors considered the authors interpretation correct. One (JM) considered that this was more likely to myocardial replacement scarring from HCM in a progressive disease phase,* and although ischemic heart disease as dual pathology was a clear possibility, it was not necessary to explain the findings. *’progressive disease’ – at any one time, 2.4-15% of HCM patients in tertiary referral centres have this phenomenon, with a >5mm increase in EDV and ESV, and >5mm wall thinning with decreased ejection fraction, often leading to heart failure.