Download
1 / 7
70 likes | 249 Views
THE COMMONWEALTH FUND. Realizing Health Reform's Potential Webinar: Health Insurance Exchanges and the Affordable Care Act of 2010 November 4, 2010. Panelists:

E N D
THE COMMONWEALTH FUND Realizing Health Reform's Potential Webinar: Health Insurance Exchanges and the Affordable Care Act of 2010November 4, 2010 Panelists: Timothy Stoltzfus Jost, J.D., Robert L. Willett Family Professor of Law, Washington and Lee University School of Law Michael T. McRaith, J.D., Director, Illinois Department of Insurance Sandra Shewry, M.P.H., M.S.W., Advisor, Health Care Reform Implementation, California Health and Human Services Agency Moderated by: Sara R. Collins, Ph.D., Vice President, The Commonwealth Fund
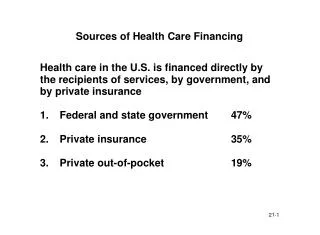
Small business tax credit • Prohibitions against lifetime benefit caps & rescissions • Phased-in ban on annual limits • Annual review of premium increases • Public reporting by insurers on share of premiums spent on non-medical costs • Preventive services coverage without cost-sharing • Young adults on parents’ plans Timeline for ACA Implementation • State insurance exchanges • Medicaid expansion • Small business tax credit increases • Insurance market reforms including no rating on health • Essential benefit standard • Premium and cost sharing credits for exchange plans • Premium increases a criteria for carrier exchange participation • Individual requirement to have insurance • Employer shared responsibility penalties • Phased-in ban on annual limits • States adopt exchange legislation and begin implementing exchanges • Penalty for individual requirement to have insurance phases in (2014-2016) • Option for state waiver to design alternative coverage programs (2017) • Insurers must spend at least 85% of premiums (large group) or 80% (small group / individual) on medical costs or provide rebates to enrollees • HHS must determine if states will have operational exchanges by 2014; if not, HHS will operate them Source: Commonwealth Fund Analysis of the The Affordable Care Act (Public Law 111-148 and 111-152).
Source of Insurance Coverage Pre-Reform and Under Affordable Care Act, 2019 23 M (8%) Uninsured 24 M (9%) Exchanges (Private Plans) 54 M (19%) Uninsured 16 M (6%) Other 16 M (6%) Other 162 M (57%) ESI 159 M (56%) ESI 10 M (4%) Nongroup 15 M (5%) Nongroup 35 M (12%) Medicaid 51 M (18%) Medicaid Pre-Reform Affordable Care Act Among 282 million people under age 65 * Employees whose employers provide coverage through the exchange are shown as covered by their employers (5 million), thus about 29 million people would be enrolled through plans in the exchange. Note: ESI is Employer-Sponsored Insurance. Source: Congressional Budget Office, Letter to Honorable Nancy Pelosi, March 20, 2010 http://cbo.gov/doc.cfm?index=11379.
ACA Provisions for Insurance Exchanges, 2014 • Each state must establish an American Health Benefit Exchange and a Small Business Health Options Program (SHOP) Exchange by 2014 for individuals and small employers; states can create single exchange; regional exchanges • If HHS determines in 2013 that a state will not have an exchange operational by 2014, HHS is required to establish and operate an exchange in the state • Individual and small-group markets not replaced by exchanges, but same market rules apply inside and outside • Non-grandfathered plans to provide essential benefit package inside/outside • Qualified health plans (QHPs) certified by exchanges; OPM to contract with carriers to offer at least two multi-state plans through exchanges, one nonprofit; $6 billion in funding for CO-OP program • QHPs must sell at least silver and gold level plans; plans selling outside can sell at any level (bronze, silver, gold, platinum) • Carriers selling inside and outside must pool risk of all enrollees • In 2014, small businesses with up to 100 employees may provide plans for their employees through exchanges, but states can limit to 50 until 2016; may open to 100+ in 2017 • Small employer tax credits (2014), premium and cost sharing subsidies, can be used only for plans purchased through the exchanges • HHS to establish permanent risk adjustment mechanism and transitional reinsurance and risk corridor programs
Federal Responsibilities for Exchanges Under ACA • Establish certification criteria and marketing requirements for QHPs • Define essential benefit package • Ensure a sufficient choice of providers including essential community providers who serve predominantly low income/medically underserved • Ensure QHPs are accredited on clinical quality measures, patient experience ratings, and other measures • Develop a uniform enrollment form for individuals and employers and present plan information in a standard format • Implement a quality improvement strategy for health plans • Provide information on quality measures on health plan performance • Develop a rating system that will rate QHPs within each benefit level on relative quality and price to be provided on the Internet portal • Establish model template for an exchange's Internet portal. The portal will be used to direct individuals/employers to QHPs, to help them determine eligibility for premium/cost-sharing credits, and present standardized information about health plans to facilitate choice • Determine initial, open, and special enrollment periods • Establish procedures to allow brokers to enroll individuals in QHPs and assist them in applying for subsidies
State Responsibilities for Exchanges Under ACA • After HHS issues regulations and sets standards for exchanges, states may adopt before Jan. 2014 the federal standard into their own laws or adopt similar standards that HHS deems equivalent • HHS will award grants, March 2011- Jan. 1 2015, to states for planning and establishing the exchanges; after that exchanges must be self-sufficient and may charge assessments or user fees to carriers or other means • Once exchange is operational state responsibilities include: • Certify qualified health plans • Operate toll-free hotline and Web site • Rate qualified health plans, present plan options in a standard format • Make recommendations on carrier participation based on past history of premium increases (as condition of premium review grants) • Inform individuals of eligibility for Medicaid and CHIP • Provide an electronic calculator to calculate plan costs • Grant certifications of exemption from individual responsibility requirement • Provide Treasury information necessary to enforce employer payments • Award grants to "navigators" to educate the public about qualified health plans, distribute information on enrollment and subsidies, facilitate enrollment, and provide referrals on grievances • In 2017, states may opt out of insurance exchanges with a 5-year waiver, if they can offer all residents coverage at least as comprehensive/affordable.
THE COMMONWEALTH FUND Questions? Visit The Commonwealth Fund at: www.commonwealthfund.org