Download
1 / 1
10 likes | 113 Views
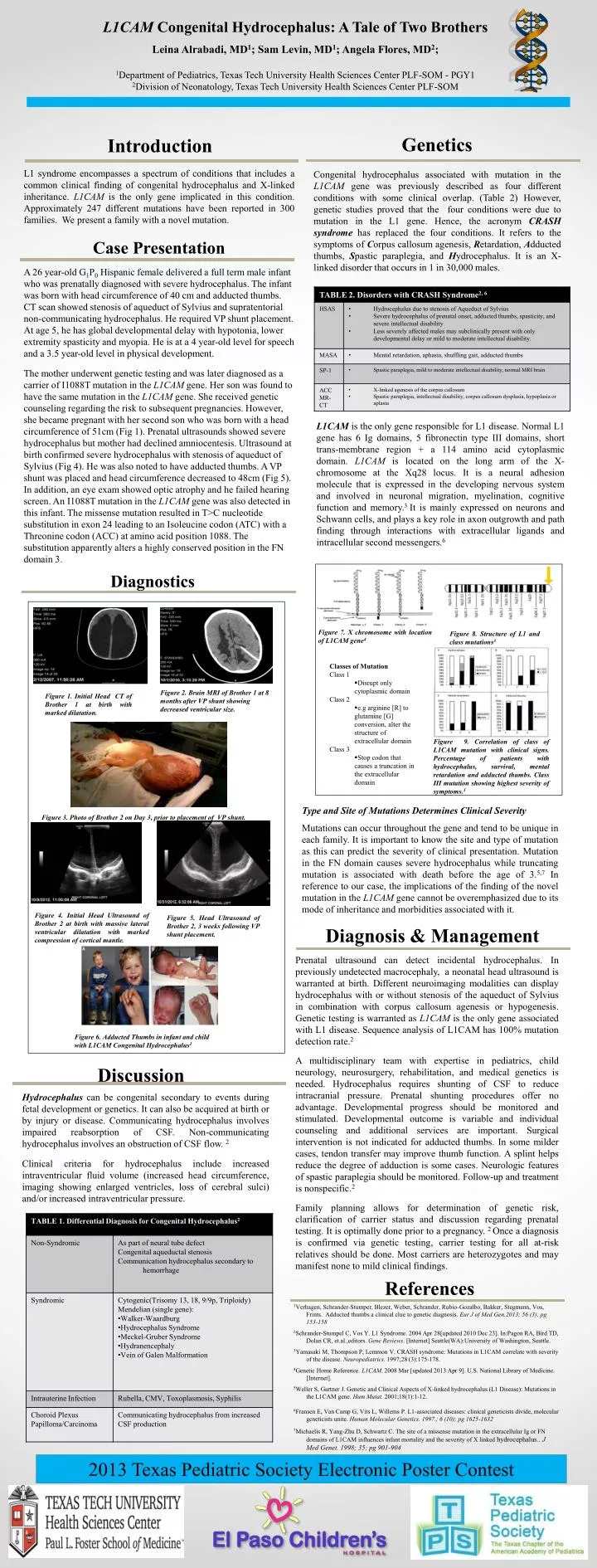
L1CAM Congenital Hydrocephalus: A Tale of Two Brothers Leina Alrabadi, MD 1 ; Sam Levin, MD 1 ; Angela Flores, MD 2 ; 1 Department of Pediatrics, Texas Tech University Health Sciences Center PLF-SOM - PGY1 2 Division of Neonatology, Texas Tech University Health Sciences Center PLF-SOM.

E N D
L1CAM Congenital Hydrocephalus: A Tale of Two Brothers Leina Alrabadi, MD1; Sam Levin, MD1; Angela Flores, MD2; 1Department of Pediatrics, Texas Tech University Health Sciences Center PLF-SOM - PGY1 2Division of Neonatology, Texas Tech University Health Sciences Center PLF-SOM Genetics Introduction Congenital hydrocephalus associated with mutation in the L1CAM gene was previously described as four different conditions with some clinical overlap. (Table 2) However, genetic studies proved that the four conditions were due to mutation in the L1 gene. Hence, the acronym CRASH syndrome has replaced the four conditions. It refers to the symptoms of Corpus callosum agenesis, Retardation, Adducted thumbs, Spastic paraplegia, and Hydrocephalus. It is an X-linked disorder that occurs in 1 in 30,000 males. L1 syndrome encompasses a spectrum of conditions that includes a common clinical finding of congenital hydrocephalus and X-linked inheritance. L1CAM is the only gene implicated in this condition. Approximately 247 different mutations have been reported in 300 families. We present a family with a novel mutation. Case Presentation A 26 year-old G1P0 Hispanic female delivered a full term male infant who was prenatally diagnosed with severe hydrocephalus. The infant was born with head circumference of 40 cm and adducted thumbs. CT scan showed stenosis of aqueduct of Sylvius and supratentorial non-communicating hydrocephalus. He required VP shunt placement. At age 5, he has global developmental delay with hypotonia, lower extremity spasticity and myopia. He is at a 4 year-old level for speech and a 3.5 year-old level in physical development. The mother underwent genetic testing and was later diagnosed as a carrier of I1088T mutation in the L1CAM gene. Her son was found to have the same mutation in the L1CAM gene. She received genetic counseling regarding the risk to subsequent pregnancies. However, she became pregnant with her second son who was born with a head circumference of 51cm (Fig 1). Prenatal ultrasounds showed severe hydrocephalus but mother had declined amniocentesis. Ultrasound at birth confirmed severe hydrocephalus with stenosis of aqueduct of Sylvius (Fig 4). He was also noted to have adducted thumbs. A VP shunt was placed and head circumference decreased to 48cm (Fig 5). In addition, an eye exam showed optic atrophy and he failed hearing screen. An I1088T mutation in the L1CAM gene was also detected in this infant. The missense mutation resulted in T>C nucleotide substitution in exon 24 leading to an Isoleucine codon (ATC) with a Threonine codon (ACC) at amino acid position 1088. The substitution apparently alters a highly conserved position in the FN domain 3. L1CAM isthe only gene responsible for L1 disease. Normal L1 gene has 6 Ig domains, 5 fibronectin type III domains, short trans-membrane region + a 114 amino acid cytoplasmic domain. L1CAM is located on the long arm of the X-chromosome at the Xq28 locus. It is a neural adhesion molecule that is expressed in the developing nervous system and involved in neuronal migration, myelination, cognitive function and memory.3 It is mainly expressed on neurons and Schwann cells, and plays a key role in axon outgrowth and path finding through interactions with extracellular ligands and intracellular second messengers.6 Diagnostics Figure 7. X chromosome with location of L1CAM gene4 Figure 8. Structure of L1 and class mutations3 • Classes of Mutation • Class 1 • Disrupt only cytoplasmic domain • Class 2 • e.g arginine [R] to glutamine [G] conversion, alter the structure of extracellular domain • Class 3 • Stop codon that causes a truncation in the extracellular domain Figure 2. Brain MRI of Brother 1 at 8 months after VP shunt showing decreased ventricular size. Figure 1. Initial Head CT of Brother 1 at birth with marked dilatation. Figure 9. Correlation of class of L1CAM mutation with clinical signs. Percentage of patients with hydrocephalus, survival, mental retardation and adducted thumbs. Class III mutation showing highest severity of symptoms.3 Type and Site of Mutations Determines Clinical Severity Mutations can occur throughout the gene and tend to be unique in each family. It is important to know the site and type of mutation as this can predict the severity of clinical presentation. Mutation in the FN domain causes severe hydrocephalus while truncating mutation is associated with death before the age of 3.5,7 In reference to our case, the implications of the finding of the novel mutation in the L1CAM gene cannot be overemphasized due to its mode of inheritance and morbidities associated with it. Figure 3. Photo of Brother 2 on Day 3, prior to placement of VP shunt. Figure 4. Initial Head Ultrasound of Brother 2 at birth with massive lateral ventricular dilatation with marked compression of cortical mantle. Figure 5. Head Ultrasound of Brother 2, 3 weeks following VP shunt placement. Diagnosis & Management Prenatal ultrasound can detect incidental hydrocephalus. In previously undetected macrocephaly, a neonatal head ultrasound is warranted at birth. Different neuroimaging modalities can display hydrocephalus with or without stenosis of the aqueduct of Sylvius in combination with corpus callosum agenesis or hypogenesis. Genetic testing is warranted as L1CAM is the only gene associated with L1 disease. Sequence analysis of L1CAM has 100% mutation detection rate.2 A multidisciplinary team with expertise in pediatrics, child neurology, neurosurgery, rehabilitation, and medical genetics is needed. Hydrocephalus requires shunting of CSF to reduce intracranial pressure. Prenatal shunting procedures offer no advantage. Developmental progress should be monitored and stimulated. Developmental outcome is variable and individual counseling and additional services are important. Surgical intervention is not indicated for adducted thumbs. In some milder cases, tendon transfer may improve thumb function. A splint helps reduce the degree of adduction is some cases. Neurologic features of spastic paraplegia should be monitored. Follow-up and treatment is nonspecific.2 Family planning allows for determination of genetic risk, clarification of carrier status and discussion regarding prenatal testing. It is optimally done prior to a pregnancy. 2 Once a diagnosis is confirmed via genetic testing, carrier testing for all at-risk relatives should be done. Most carriers are heterozygotes and may manifest none to mild clinical findings. Figure 6. Adducted Thumbs in infant and child with L1CAM Congenital Hydrocephalus1 Discussion Hydrocephalus can be congenital secondary to events during fetal development or genetics. It can also be acquired at birth or by injury or disease. Communicating hydrocephalus involves impaired reabsorption of CSF. Non-communicating hydrocephalus involves an obstruction of CSF flow. 2 Clinical criteria for hydrocephalus include increased intraventricular fluid volume (increased head circumference, imaging showing enlarged ventricles, loss of cerebral sulci) and/or increased intraventricular pressure. References 1Verhagen, Schrander-Stumper, Blezer, Weber, Schrander, Rubio-Gozalbo, Bakker, Stegmann, Vos, Frints. Adducted thumbs a clinical clue to genetic diagnosis. Eur J of Med Gen.2013; 56 (3); pg 153-158 2Schrander-Stumpel C, Vos Y. L1 Syndrome. 2004 Apr 28[updated 2010 Dec 23]. In:Pagon RA, Bird TD, Dolan CR, et.al.,editors. Gene Reviews. [Internet] Seattle(WA):University of Washington, Seattle. 3Yamasaki M, Thompson P, Lemmon V. CRASH syndrome: Mutations in L1CAM correlate with severity of the disease. Neuropediatrics. 1997;28 (3):175-178. 4Genetic Home Reference. L1CAM. 2008 Mar [updated 2013 Apr 9]. U.S. National Library of Medicine. [Internet]. 5Weller S, Gartner J. Genetic and Clinical Aspects of X-linked hydrocephalus (L1 Disease): Mutations in the L1CAM gene. Hum Mutat. 2001;18(1):1-12. 6Fransen E, Van Camp G, Vits L, Willems P. L1-associated diseases: clinical geneticists divide, molecular geneticists unite. Human Molecular Genetics. 1997.; 6 (10); pg 1625-1632 7Michaelis R, Yang-Zhu D, Schwartz C. The site of a missense mutation in the extracellular Ig or FN domains of L1CAM influences infant mortality and the severity of X linked hydrocephalus.. J Med Genet. 1998; 35; pg 901-904 2013 Texas Pediatric Society Electronic Poster Contest






